GO BACK
From my hands-on experience working with cardiology practices, I’ve seen how often CPT code 78452 becomes a source of confusion for medical billing teams and a loss of revenue for doctors. Many healthcare providers perform the test correctly and document the study, but still face claim rejections. The most common problem is confusion between 78451 and 78452.
In several cases, cardiology practices are losing thousands of dollars simply because the technical and professional components were billed incorrectly, or the ICD-10 code did not fully support medical necessity. These are not rare issues. They happen every week in real medical billing workflows.
To overcome this issue, this blog is written from a billing and compliance perspective, not just a textbook definition. It explains what CPT code 78452 really includes, how payers review it, and how to document and bill it correctly.
What is 78452 CPT Code?
CPT code 78452 is a nuclear medicine procedure used for myocardial perfusion imaging (MPI). It evaluates how well blood flows through the heart muscle using single-photon emission computed tomography (SPECT).
The term “SPECT mult” indicates multiple images obtained during both a rest phase and a stress phase. These image sets allow healthcare providers to compare blood flow under different conditions and identify abnormalities.
In cardiology practice, CPT 78452 is most often used in nuclear cardiology labs and hospital outpatient departments to diagnose coronary artery disease (CAD) and evaluate treatment effectiveness.
The Clinical Purpose of CPT 78452
The clinical purpose of the 78452 CPT code is to identify ischemia, infarction, and other cardiac problems related to decreased myocardial blood flow. It helps determine myocardial viability, detect areas of cardiac injury and also helps the insurance payer to check for approval criteria.
Practical Examples of CPT 78452 Use
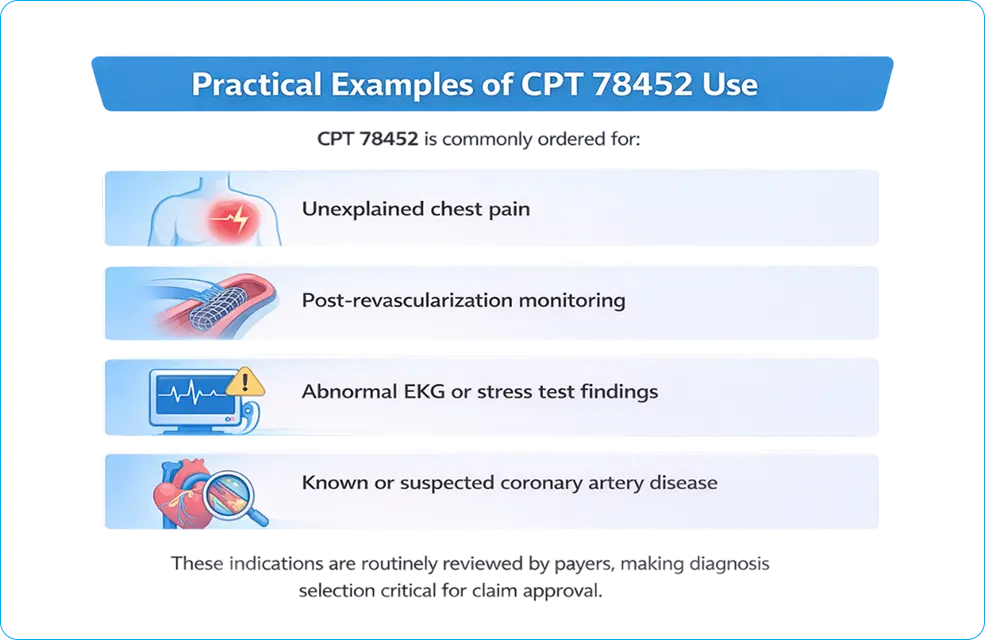
CPT 78452 is commonly ordered for:
- Unexplained chest pain
- Post-revascularization monitoring
- Abnormal EKG or stress test findings
- Known or suspected coronary artery disease
These indications are routinely reviewed by payers, making diagnosis selection critical for claim approval.
ICD-10 Codes Supporting Medical Necessity for CPT 78452
Correct ICD-10 linkage is one of the most common difficulties for cardiology practices and billing teams. Frequently accepted diagnosis codes include:
- R07.2 – Precordial chest pain
- I25.10 – Atherosclerotic heart disease
- I20.9 – Angina pectoris
- R94.31 – Abnormal EKG
- Z95.5 – Presence of coronary angioplasty implant
- Z86.79 – Personal history of CAD
Incomplete or mismatched diagnosis coding is a leading cause of denials, underpayments, and payer audits for CPT 78452.
Clinical Protocol for CPT 78452
Before the test, patients usually have to fast and have their medications checked. Some medications may be temporarily withheld to ensure accurate results.
Clinical factors like diabetes, high blood pressure, COPD, or arthritis help decide if exercise stress or drug stress is the best choice. Proper preparation helps with both clinical accuracy and the ability to defend documentation during payer review.
Step-by-Step Procedure
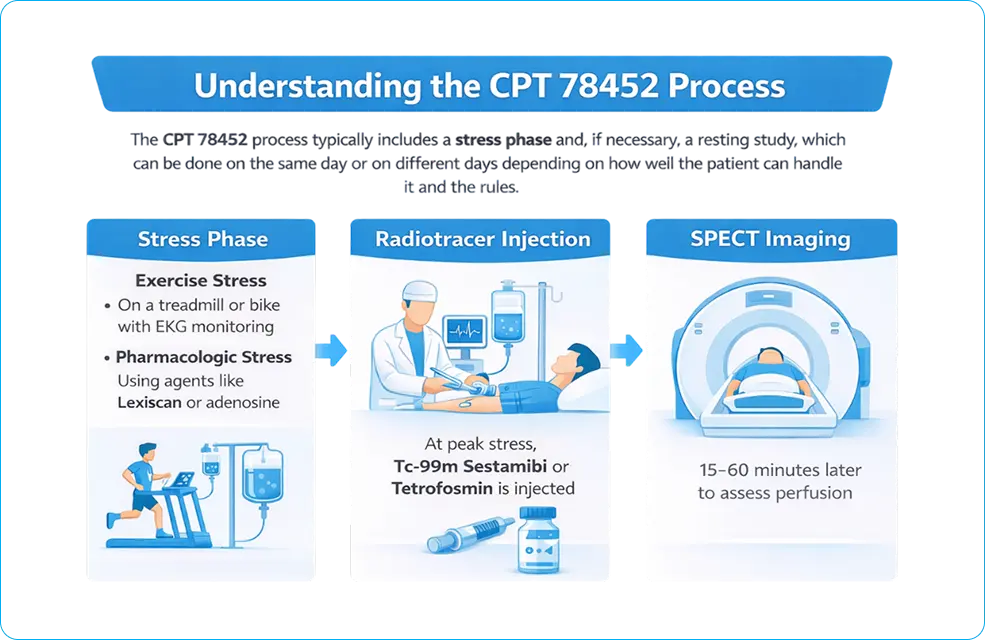
The CPT 78452 process has a stress phase and, if necessary, a resting study. These can happen on the same day or on different days, depending on how well the patient can handle it and the rules.
During the stress phase, myocardial blood flow is increased using:
- Exercise stress, like testing on a treadmill or bike, while keeping an eye on the patient’s heart rate with an EKG
- Pharmacologic stress, employing agents such as Lexiscan (regadenoson) or adenosine
- At the height of stress, a radiotracer like technetium-99m sestamibi or tetrofosmin is injected.
- SPECT imaging is done about 15 to 60 minutes after the injection to check perfusion.
SPECT Imaging
SPECT imaging makes 3D pictures of the heart that can be used to measure and describe its condition. These pictures help find problems with blood flow, look at the heart’s structure, and check how well the heart is working overall.
Study at Rest Position
The resting study looks at blood flow in the heart without any stress. CPT 78451 with modifier -52 may apply if only one imaging phase is finished or services are cut back. For compliance, it is important to be able to tell the difference between one study and many studies.
CPT Code 78452 Includes:
- Stress and rest imaging phases
- Giving radiopharmaceuticals
- Getting and processing SPECT images
- Seeing blood flow
- Interpretation by a doctor and diagnostic reporting
As a whole, these parts make up a single nuclear cardiology service.
78452 vs 78451: Key Differences and Examples
CPT 78452 is for more than one imaging study, while CPT 78451 is only for one imaging study. Some common situations are:
- Stress and rest imaging done in one session
- Stress imaging is performed first, followed by rest imaging
- Incomplete rest imaging is charged as fewer services
- Billing mistakes and lost money are common when these codes are used incorrectly.
CPT 78451 has fewer images and is less complicated. CPT 78452 needs more imaging, a more thorough interpretation, and helps with a full cardiac assessment. These differences have a direct impact on reimbursement and audit risk.
Revenue Optimization Strategy for CPT 78452: From Claim to Cash
CPT code 78452 is not just a diagnostic service—it is a high-value revenue driver in cardiology billing. Practices that treat it as a structured financial workflow instead of a single claim achieve higher reimbursement consistency and lower denial rates.
Revenue Leakage Points in 78452 Billing
Most financial loss does not come from outright denials—it comes from silent inefficiencies:
- Under-coded services (missing -26 or -TC split billing)
- Incorrect ICD-10 sequencing reducing medical necessity strength
- Missed drug reimbursement (e.g., J2785 for Lexiscan)
- Bundling errors under National Correct Coding Initiative edits
- Failure to track payer-specific reimbursement variance
These issues reduce net collection per study even when claims are technically “paid.”
End-to-End Revenue Optimization Framework
A structured approach aligns clinical workflow with payer expectations and financial outcomes:
| Stage | Action | Revenue Impact |
|---|---|---|
| Pre-Visit | Verify eligibility + authorization | Prevents upfront denial |
| Clinical | Capture risk factors + prior testing | Strengthens medical necessity |
| Coding | Align CPT + ICD + modifiers | Improves first-pass rate |
| Billing | Apply payer-specific rules | Reduces rework |
| Post-Submission | Track ERA/EOB variance | Identifies underpayment |
| Audit | Internal compliance review | Prevents recoupments |
RPM (Revenue Per Study) Optimization Drivers
Practices that actively monitor these variables outperform others:
- Modifier accuracy rate (%)
- First-pass claim acceptance rate
- Average reimbursement variance by payer
- Denial rate for nuclear cardiology services
- Turnaround time (DOS → Payment)
Even a 5–8% improvement in clean claim rate for CPT 78452 can translate into thousands of dollars monthly for mid-size cardiology groups.
Payer Contract Leverage Strategy
High-volume imaging codes like 78452 can be used to renegotiate contracts:
- Compare allowed amounts across payers
- Identify underperforming contracts
- Use utilization data as negotiation leverage
- Align reimbursement with Centers for Medicare & Medicaid Services benchmarks
Operational Insight
Practices that integrate clinical documentation → coding accuracy → payer logic → financial tracking operate with a closed-loop revenue system.
This eliminates guesswork and transforms CPT 78452 from a high-risk audit code into a predictable revenue stream.
Billing Rules for the 78452 CPT Code
To bill CPT 78452 correctly, you need to pay close attention to payer policies, how to use modifiers, and documentation standards. Mistakes in this area often result in payments being denied or delayed.
Documentation Checklist
- ICD-10 clinical indication
- Symptoms and risk factors for the patient
- Method of stress used
- Radiopharmaceutical given
- Timing and phases of imaging
- Final report and interpretation
How Do Payers Decide to Approve or Deny CPT 78452?
Payers do not evaluate CPT Code 78452 based on the procedure alone. Approval depends on how clinical data supports medical necessity and risk evaluation.
Payer Decision Logic Framework
Payers apply a structured review model across four variables:
1. Symptom Severity and Presentation
- Typical angina (exertional chest pain, radiating discomfort) → strong approval signal
- Atypical chest pain → conditional approval
- No symptoms → high denial probability
2. Prior Diagnostic Testing
- Abnormal Electrocardiogram → supports medical necessity
- Inconclusive stress test → justifies advanced imaging
- No prior testing → weak justification
3. Risk Stratification (CAD Probability)
- High-risk patients (diabetes, hypertension, smoking history) → approved
- Intermediate risk → conditional (documentation-dependent)
- Low-risk or screening use → denied
4. ICD-10 Alignment with Medical Necessity
- Covered diagnoses (e.g., angina, ischemic heart disease) → approved
- Non-specific symptoms (fatigue, general weakness) → denied
- Mismatch between diagnosis and test purpose → denial trigger
Example Payer Decision Flow
| Clinical Scenario | Payer Outcome |
| Stable chest pain with risk factors | Approved |
| Abnormal ECG + suspected ischemia | Approved |
| Asymptomatic screening | Denied |
| No prior testing + vague symptoms | Denied |
Payers evaluate clinical pathway logic, not just documentation presence. If the test does not logically follow prior findings, the claim fails.
When Does CPT 78452 Require Prior Authorization?
Authorization requirements depend on payer type. The same procedure can be auto-approved, conditionally approved, or strictly denied based on plan rules.
Medicare vs Medicare Advantage
| Payer Type | Authorization Requirement |
|---|---|
| Traditional Medicare | Usually not required |
| Medicare Advantage | Often required (plan-specific rules apply) |
Commercial Payer Authorization Rules
Major payers such as Aetna and Humana apply strict utilization controls.
Authorization is required when:
- Test is not preceded by basic diagnostics
- Symptoms are non-specific
- Frequency exceeds payer thresholds
Required Documentation for Approval
Authorization depends on structured clinical evidence:
- Clinical notes describing chest pain characteristics
- Prior test results (ECG, stress test, echocardiogram)
- Documented failure or limitation of initial testing
- Risk factors (age, diabetes, hypertension, CAD history)
Operational Gap:
Missing prior test documentation is one of the most common reasons for pre-authorization denial.
CPT 78452 Modifiers
Some common modifiers are;
- 26: Professional part (interpretation and report)
- TC stands for technical component, which includes imaging and equipment.
- 52: Fewer services
- 59: Separate procedural service
Does CPT 78452 Need a Modifier?
Modifier use depends on the billing context. Modifiers -26, -TC, -59, -76, -77, -91, or -99 may apply based on repeat services or multiple procedures. Clear documentation is essential to avoid audits. Each modifier must be clearly supported in the medical record.
Related CPT Codes
Related codes include CPT 78451, CPT 78454, and CPT 78480. PET imaging requires different codes and documentation.
Bundling Rules
Services such as stress testing (CPT 93015 or 93017) and pharmacologic agents like J2785 (Lexiscan) must be reviewed carefully to avoid incorrect unbundling.
NCCI Bundling & Compliance Rules
NCCI edits define which services are bundled and which may be reported separately. Failure to follow NCCI rules exposes practices to post-payment audits and recoupments.
What Is Included vs NOT Included in CPT Code 78452
Included services:
- Stress and rest SPECT image acquisition
- Image processing and reconstruction
- Blood flow assessment
- Physician interpretation and report
- Heart–lung ratio calculation when part of MPI
Not separately reportable:
- 78580 when performed only as part of MPI
- IV access solely for tracer injection
- Routine monitoring is inherent to the procedure
Global vs Split Billing
- Global billing applies when one entity performs all components
- Split billing applies when facilities bill technical services and physicians bill interpretation using -26 and -TC.
Lexiscan (Regadenoson) Coding
Lexiscan (regadenoson) is billed with J2785 at 0.4 mg / 5 mL. Side effects such as flushing or shortness of breath should be documented to support medical need and drug reimbursement.
Real-World Billing & Claim Examples
In office-based cardiology practices, missing modifiers are common. In hospital settings, split-billing errors occur more often. Addressing these issues improves first-pass claim acceptance.
Medicare Reimbursement Policy for CPT 78452
The amount of money Medicare pays back depends on the case, where the person lives, and how well the documentation is done. Medicare Part B pays for drugs, and professional and technical services are paid for separately.
How much will Medicare pay for CPT Code 78452?
The Medicare Physician Fee Schedule (MPFS) and MAC (Medicare Administrative Contractor) specific rules set the payment amount. Rates change from year to year and from place to place.
The quality of the documentation, the rules of the payer, and the medical necessity all affect reimbursement. If you don’t have enough evidence or modifiers, you may not get paid, or your claim may be denied. Many Medicare Advantage plans and private insurers like Humana and Aetna need you to get permission first. If you don’t get approval, your claim could be denied.
Audit Risk Areas for CPT 78452
Audit exposure increases when billing patterns do not match clinical necessity. Payers and auditors target high-cost imaging codes like CPT Code 78452 for compliance review.
High-Risk Audit Triggers
1. Overutilization Without Clinical Indication
- Frequent MPI orders without documented symptoms
- Screening use without risk stratification
2. Missing Stress Test Documentation
- No record of stress method (exercise or pharmacologic)
- Incomplete imaging phases (rest vs stress)
3. Incorrect Modifier Usage
- Missing or incorrect use of -26 (professional) or -TC (technical)
- Global billing without facility alignment
4. Unbundling Violations
- Separately billing components included in 78452
- Duplicate reporting of related imaging services
Common 78452 Denials and How to Fix Them
Some common reasons for denial are not enough medical evidence, missing modifiers, and mistakes in bundling. Fixing these problems will help you lose less money. Some steps to take to avoid problems are:
- checking the diagnosis
- accuracy of modifiers
- internal audits to keep payments from being late.
Conclusion
After working through countless nuclear stress test claims, payer denials, and delayed payments, one thing is clear: CPT code 78452 is not simple, even though many resources describe it that way.
From real billing experience, most reimbursement issues tied to 78452 are preventable. When documentation, modifier selection, unbundling, and ICD-10 linkage are handled correctly, approval rates improve, and audit risk drops significantly.
Accurate use of CPT code 78452 requires more than knowing the definition. To do this, you need to know what the clinical intent is and what the payer expects. Moreover, the NCCI rules and how Medicare and private insurers really look at these claims are also important. Practices that use this level of accuracy have fewer denials, more reliable payments, and better financial stability.
This guide is based on real-world experience, not theory. It is meant to help cardiology providers, billing teams, and compliance professionals code and bill CPT 78452 with confidence, knowing that their claims are legal, correct, and ready for an audit.
FAQs
Frequently asked questions about the 78452 CPT code use are:
What is CPT code 78452 for?
CPT code 78452 is used for myocardial imaging and PET.
When should 78452 not be billed?
CPT 78452 should not be billed when only a single-phase study is performed (use 78451), when documentation does not support medical necessity, or when services are bundled under National Correct Coding Initiative edits.
Can 78452 be repeated?
CPT 78452 can be repeated only when medically necessary (e.g., new symptoms or inadequate prior study) and must be supported with proper documentation and appropriate modifiers.
What documentation do auditors check?
Auditors verify clinical indication (ICD-10), stress method, radiotracer details, imaging phases (rest + stress), timing, and the final physician interpretation/report aligned with Centers for Medicare & Medicaid Services guidelines.
Is CPT 78452 covered by Medicare?
Yes! It is reimbursed by Medicare.
Is CPT code 78452 a PET scan?
No, CPT 78452 is used for SPECT myocardial perfusion imaging, not PET scan.
What is the difference between 78452 and 78454?
78452 specifies the tomographic (SPECT), including attenuation correction, while 78454 states planar. So the distinction is the type of imaging and the type of camera used.
Can you bill for two CPT codes at the same time?
Yes! It is possible to bill 2 CPT codes at the same time fram,e depending upon the medical conditions found.
Are You Being Underpaid for the 78452 CPT Code?
Underpayments may occur due to contract terms, modifier errors, or payer processing issues.