GO BACK
Authorization-related denials occur when a healthcare service requires prior payer approval, but the claim lacks a valid authorization, or the approval details do not match the billed service. These denials originate from gaps in scheduling, insurance verification, or coding workflows.
This guide explains how authorization denials occur, the denial reasons, payer policy factors, correction and appeal options, and workflow strategies clinics use to prevent authorization-related claim denials.
What Are Authorization-Related Denials in Medical Billing?
Authorization-related denials are payer denials issued when a claim requires pre-service approval and the payer cannot validate authorization at adjudication. Denials occur in two situations:
- No valid authorization exists for the billed service
- Authorization exists but does not match the claim (code, units, provider, location, or date window)
These denials are utilization management outcomes, not claim formatting errors. Fixing them requires identifying which approval rule was violated and whether the payer allows resubmission, appeal, or retroactive authorization.
What Is Prior Authorization and Why Do Payers Require It?
Prior authorization is the payer’s requirement for pre-service approval before specific services are performed. Payers use it to confirm medical necessity and control utilization for certain services
Prior authorization validates:
- the requested CPT/HCPCS and planned service type
- The diagnosis supporting medical necessity
- the provider NPI and service location
- the units/quantity and valid date range
Authorization Types in Medical Billing
Prior (Prospective) Authorization (PA):
Often called pre-authorization, this is approval required from the insurer before performing non-emergency services, such as specific procedures, imaging, or medications.
Concurrent Authorization:
Occurs during an ongoing treatment or inpatient stay, ensuring continued necessity for services like extended hospital stays or rehab.
Retrospective Authorization:
Sought after services have been provided, commonly used for emergency room visits or urgent, unavoidable medical situations.
Referral Authorization:
A formally documented approval for a patient to see a specialist, typically initiated by a Primary Care Provider (PCP).
Step Therapy Authorization:
A type of prior authorization for medication, requiring patients to try a lower-cost, safer drug before the insurer covers a more expensive one.
Why Authorization Matters
Payment Security: Helps avoid claim denials (e.g., CO 197), which indicate that a required pre-authorization was not completed.Medical Necessity: Confirms the treatment is medically necessary.Cost Control: Helps insurers track and regulate expensive treatments.
What Is the Difference Between Pre-Certification and Prior Authorization?
Pre-certification and prior authorization are approval processes used by insurers before certain services are performed. Some payers use the terms interchangeably, but they represent different review stages within utilization management.
| Aspect | Pre-Certification | Prior Authorization |
| Primary purpose | Confirms the service is eligible under the patient’s insurance plan | Confirms the service meets medical necessity criteria |
| Review type | Administrative coverage validation | Clinical utilization review |
| What is evaluated | Plan benefits, eligibility, service category | CPT/HCPCS code, diagnosis, treatment necessity |
| Approval scope | Confirms that the treatment episode is covered | Approves the specific service details to be billed |
| Typical documentation | Basic patient and plan information | Clinical notes, diagnosis codes, treatment justification |
In billing workflows, pre-certification verifies plan eligibility, while prior authorization approves the exact service parameters, including CPT code, provider, location, service date, and authorized units.
Clinics should record the authorization reference number, approval scope, and validity dates before the service is performed.
How Does the Prior Authorization Process Work Before Patient Treatment?
The prior authorization process occurs before a healthcare service is delivered. Clinics must confirm whether authorization is required, submit clinical documentation to the payer, and receive approval before the scheduled service date, or the insurer denies reimbursement.
A typical prior authorization workflow includes the following steps:
| Step | Authorization Activity | Operational Purpose |
| Authorization requirement check | Verify payer policy and CPT/HCPCS requirements | Identify services requiring approval |
| Clinical documentation preparation | Gather diagnosis codes, treatment notes, and justification | Support medical necessity review |
| Authorization submission | Submit request through payer portal, clearinghouse, or phone | Initiate payer review |
| Payer clinical review | Utilization management evaluates necessity and coverage | Approve or deny request |
| Authorization approval issued | Payer assigns authorization reference number | Enables service delivery and billing |
For What Services Must Clinics Obtain Prior Authorization?
Insurers require prior authorization for services that carry higher cost, utilization risk, or specialized treatment criteria.
Services requiring authorization include:
- Elective surgical procedures
- Advanced diagnostic imaging (MRI, CT, PET scans)
- Specialty referrals and consultations
- Inpatient hospital admissions
- Certain outpatient procedures and therapies
Most insurers publish authorization requirement lists based on CPT or HCPCS codes. These lists must be checked during scheduling or insurance verification to ensure authorization requests are submitted before treatment.
What Information Must Match the Authorization Approval?
Authorization approvals are tied to specific claim attributes. For reimbursement to occur, the submitted claim must match the authorization record exactly.
Key authorization elements include:
| Authorization Element | Why It Matters |
| CPT or HCPCS procedure code | Confirms the approved service |
| Diagnosis code | Supports medical necessity review |
| Provider NPI | Authorization linked to a specific clinician |
| Service location or facility | Some approvals apply only to a specific site |
| Authorized units or quantity | Ensures the billed volume matches approval |
| Authorization validity dates | Service must occur within the approved timeframe |
| Authorization reference number | Required identifier on the claim |
If any of these elements differ between the authorization record and the claim submission, the payer classify the claim as unauthorized and deny payment.
How Does Drug Prior Authorization Work?
Drug prior authorization applies to prescription medications that require payer approval before coverage is granted. These rules are commonly applied to high-cost drugs, specialty medications, or treatments with multiple therapeutic alternatives.
To request approval, the prescribing provider must submit clinical information such as:
- Diagnosis codes
- Treatment history or prior therapies
- Medication dosage and duration
- Clinical justification for the drug/rationale
Pharmacy benefit managers (PBMs) or payer pharmacy departments review this information against formulary policies and medical necessity criteria for each benefit plan.
Drug authorization decisions involve:
- Step therapy requirements
- Quantity limits
- Formulary restrictions
If approved, the payer assigns an authorization reference number, allowing the pharmacy claim to process under the patient’s insurance plan.
When authorization is not obtained before dispensing the medication, the pharmacy claim gets rejected and the patient have to pay out of pocket.
What Are the Ways Prior Authorization Is Performed?
Clinics submit prior authorization requests through multiple operational channels depending on payer technology and internal workflow. The objective is to transmit clinical documentation, obtain payer approval, and record the authorization reference number before the service is performed.
Most clinics rely on payer portals, clearinghouse tools, EHR-integrated systems, or direct communication with utilization management departments.
| Authorization Method | How It Works | Use Case |
| Payer Portal Submission | Staff submit authorization requests and upload clinical documentation directly in the insurer’s provider portal | Imaging services, elective procedures |
| Clearinghouse Authorization Tools | Authorization requests are submitted through billing software or clearinghouse integrations | High-volume clinics managing multiple payers |
| Phone Authorization | Staff contact the payer’s utilization management department to request approval | Urgent or same-day services |
| EHR-Integrated Authorization | Authorization requests and approvals are tracked directly within the electronic health record | Large health systems with integrated workflows |
| Delegated Utilization Vendors | Third-party utilization management organizations review authorization requests on behalf of insurers | Managed care plans and specialty procedures |
These methods allow clinics to submit authorization requests, track approval status, and maintain documentation required for claim submission.
Major Insurance Authorization Portals
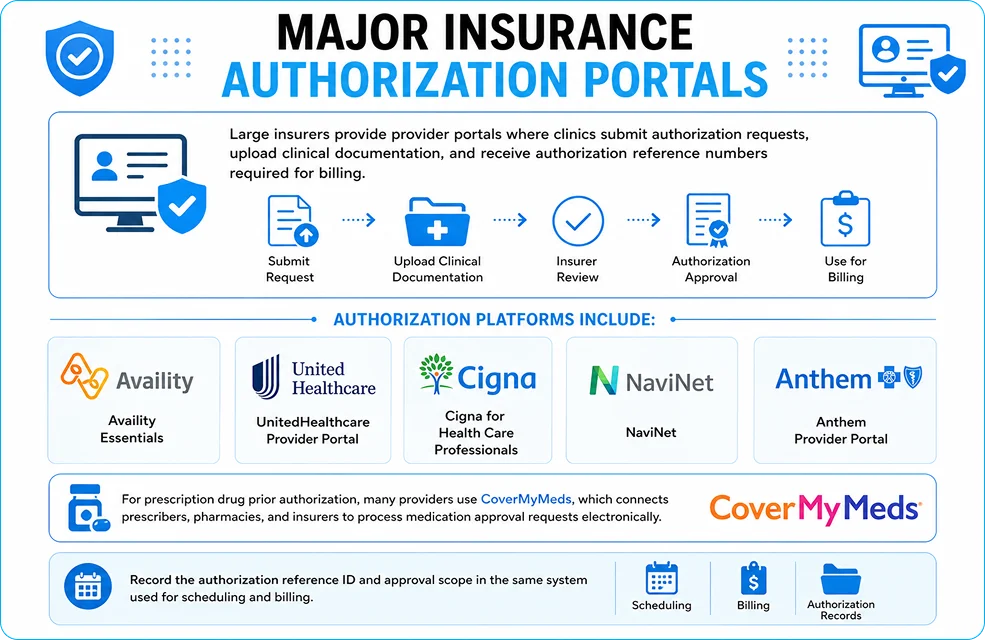
Large insurers provide provider portals where clinics submit authorization requests, upload clinical documentation, and receive authorization reference numbers required for billing.
Authorization platforms include:
- Availity Essentials
- UnitedHealthcare Provider Portal
- Cigna for Health Care Professionals
- NaviNet
- Anthem Provider Portal
For prescription drug prior authorization, many providers use CoverMyMeds, which connects prescribers, pharmacies, and insurers to process medication approval requests electronically.
Record the authorization reference ID and approval scope in the same system used for scheduling and billing.
What Are the Authorization-Related Claim Denial Reasons?
Authorization denials occur when the payer cannot validate a prior approval for the billed service or when the authorization details do not match the submitted claim. These denials usually originate from workflow failures during scheduling, coding validation, or insurance verification.
| Denial Reason | What Happens | Typical Workflow Failure |
| Missing or Invalid Prior Authorization | Service requires authorization but none was obtained before treatment | Authorization requirement not verified during scheduling |
| Incorrect CPT / HCPCS Code Authorization | Authorization approved for a different procedure than the one billed | Coding or procedure change not updated in authorization request |
| Authorization Expired Before Service Date | Service performed outside the approved authorization timeframe | Scheduling changes without updating authorization |
| Units Authorized Do Not Match Units Billed | Claim exceeds the number of sessions or units approved | Billing more services than the authorization allowed |
| Referral or In-Network Provider Violation | Required referral missing or provider outside network | Referral verification failure during intake |
| Observation vs Inpatient Authorization Mismatch | Authorization approved for one care level but claim billed under another | Admission status changed without updating authorization |
These denial categories represent predictable operational breakdowns in pre-service workflows.Track these reasons by payer and service line to target the workflow step causing the mismatch.
What Denial Codes Indicate Authorization Problems?
Insurance payers use Claim Adjustment Reason Codes (CARC) to indicate why a claim was denied. These standardized denial codes help professional billing teams identify authorization failures and determine whether the claim should be corrected, resubmitted, or appealed.
| Denial Code | Meaning | Typical Cause |
| CO-197 | Authorization required for this service | Prior authorization not obtained |
| CO-198 | Authorization invalid or expired | Service performed outside approval dates |
| CO-204 | Service not covered under plan | Authorization does not align with benefit rules |
| CO-96 | Non-covered service | Authorization mismatch or coverage limitation |
| CO-109 | Claim not covered by payer | Incorrect payer, referral requirement, or plan issue |
Authorization denial codes guide claim resolution by indicating whether the claim should be corrected and resubmitted, appealed with supporting documentation, or adjusted based on payer liability rules.
How Do Authorization Errors Occur in the Clinical Scheduling Workflow?
Authorization failures originate during pre-service scheduling and insurance verification. When authorization requirements are not validated before treatment, clinics perform services without payer approval, resulting in claim denials.
| Scheduling Error | What Happens | Workflow Gap |
| Authorization not verified | Service performed without approval | Authorization requirement not checked during scheduling |
| Treatment plan change | Approved procedure differs from billed service | Updated authorization not obtained |
| Facility vs professional authorization confusion | Only one service component approved | Separate approvals required |
| Authorization tied to specific provider | Claim submitted under different NPI | Provider mismatch |
Integrating authorization checks into scheduling and insurance verification workflows prevents these avoidable denials.
How Do Payer Policies and Utilization Management Vendors Affect Authorization?
Authorization policies vary by insurer and involve utilization management (UM) programs that review medical necessity before approving services. Many insurers also delegate authorization reviews to external vendors.
| Authorization Factor | Impact on Claims |
| Delegated utilization management vendors | Providers must follow vendor submission and review procedures |
| Diagnosis-specific authorization rules | Authorization valid only for approved diagnosis codes |
| Multi-service procedures | Separate approvals required for each service component |
| Outpatient vs inpatient pathways | Different authorization rules depending on care setting |
Understanding payer-specific authorization policies helps clinics submit accurate authorization requests and avoid denials.
How Should Clinics Correct Authorization-Related Denials?
Correcting authorization denials requires identifying the root cause and determining whether the claim should be corrected and resubmitted or formally appealed.
| Correction Method | When It Applies | Required Action |
| Retroactive authorization request | Payer allows post-service approval | Submit request with clinical justification within payer deadlines |
| Claim correction and resubmission | Authorization exists but claim details do not match | Correct CPT code, provider NPI, or service date and resubmit |
| Formal appeal submission | Payer denies authorization despite medical necessity | Provide supporting clinical documentation |
| Peer-to-peer medical review | Payer requires physician-level justification | Treating physician discusses case with payer medical reviewer |
Appeals include clinical notes, diagnosis documentation, treatment rationale, and policy references demonstrating that the service met payer medical necessity criteria.
If the appeal is approved, the payer reprocesses the claim and issues payment. If denied, the balance move to contractual adjustment or patient liability depending on plan rules.
How Can Clinics Prevent Authorization-Related Claim Denials?
Preventing authorization denials depends on consistent pre-service verification, standardized documentation, and clear workflow controls.
Clinics improve authorization performance by verifying payer requirements early, submitting complete documentation, and ensuring authorization reference numbers are included in claim submission. Standardized processes reduce errors that lead to authorization-related denials.
What Are the Best Workflow Checkpoints to Prevent Authorization Denials?
Structured checkpoints ensure that authorization requirements are validated, approvals remain valid, and claim details match payer authorization before submission.
| Workflow Stage | Authorization Check |
| Scheduling | Confirm whether the planned service requires prior authorization based on CPT/HCPCS requirements |
| Insurance verification | Validate payer policies, referral rules, and coverage eligibility |
| Pre-service review | Confirm CPT/HCPCS codes, authorized units, provider NPI, and service location match the approval |
| Authorization monitoring | Track authorization validity dates and expiration before the service occurs |
| Authorization tracking systems | Use EHR or authorization tracking tools to monitor approval status and approved services |
| Pre-billing review | Ensure the authorization reference number and approval details are attached to the claim |
| Claim submission | Verify authorization data is transmitted correctly with the claim |
| Documentation control | Maintain an audit trail of authorization approvals, payer responses, and supporting documentation |
What Technology Helps Reduce Authorization Denials?
Technology enforces authorization controls at scale by automating requests, flagging risk, and tracking payer policy changes.
| Technology Capability | How It Reduces Authorization Denials |
| Authorization workflow automation | Routes authorization requests, tracks approval status, and generates alerts when approvals approach expiration |
| Predictive denial analytics | Identifies claims likely to deny based on historical payer behavior and authorization patterns |
| Payer policy monitoring tools | Track policy updates across insurers so clinics can adjust authorization workflows before requirements change |
What Financial Risks Occur When Services Are Performed Without Authorization?
Performing services without required authorization exposes healthcare providers to reimbursement loss and compliance risks. When authorization is missing or invalid, insurers deny the claim and shift financial responsibility based on plan rules and contractual terms.
| Financial Risk | Impact on Providers |
| Patient vs insurance liability (CO vs PR codes) | Adjustment codes determine whether the provider must write off the charge (CO) or bill the patient (PR) |
| Contract-specific authorization requirements | Some payer contracts require authorization even when the general policy appears flexible |
| Revenue loss and administrative cost | Denials increase rework, appeals, and write-off risk |
| Compliance and audit exposure | Repeated authorization failures trigger payer audits or contractual reviews |
| Value-based care compliance | Authorization controls help ensure services align with care management and utilization policies |
Failure to follow authorization requirements can therefore result in lost reimbursement, increased operational cost, and contractual compliance risks for healthcare providers.
Conclusion
Authorization-related denials are largely preventable when clinics treat prior authorization as a structured pre-service control rather than a billing task. Verifying payer requirements during scheduling, aligning service details with approval parameters, and maintaining clear authorization documentation reduce avoidable claim failures.
Healthcare organizations that implement defined workflows, monitor payer policy changes, and integrate authorization tracking into clinical and billing systems improve claim accuracy and reimbursement stability. A disciplined authorization process ultimately protects revenue, reduces administrative rework, and strengthens overall revenue cycle performance.
Frequently Asked Questions About Authorization Denials
What is the difference between a referral and prior authorization?
A referral is a primary care provider’s approval for a patient to see a specialist, usually required in HMO plans. Prior authorization is insurer approval confirming that a specific medical service or procedure meets coverage and medical necessity requirements.
What triggers prior authorization requirements?
Prior authorization is required for high-cost services, advanced imaging, specialty medications, inpatient admissions, and certain elective procedures. Insurers identify these services through CPT or HCPCS code authorization lists.
Can insurance approve authorization retroactively?
Some insurers allow retroactive authorization when medical necessity is documented, but approval is not guaranteed. Requests must usually be submitted within strict payer timelines and supported by clinical documentation.
What happens if a service is performed without prior authorization?
If authorization was required but not obtained, the insurer denies the claim. Depending on payer rules and contract terms, the cost shift to the provider as a write-off or to the patient as financial responsibility.
How long does a prior authorization remain valid?
Authorization approvals remain valid for a limited timeframe defined by the payer. The service must occur within the approved date range and match the authorized procedure, provider, and service location.
What services commonly require prior authorization?
Services requiring authorization include MRI and CT scans, elective surgical procedures, specialty medications, inpatient admissions, and certain outpatient treatments.
Who is responsible for obtaining prior authorization in medical billing?
Prior authorization responsibilities are shared across scheduling staff, insurance verification teams, clinical providers, and billing personnel. Clear role assignment ensures authorization requests are submitted, approved, and correctly linked to claims before treatment occurs.