Practices typically manage billing in two ways: an in-house team or an outsourced medical billing company. This page compares staffing, technology, ROI, compliance risk, and scalability so providers can choose the setup that fits their operations and growth plans.
What Is Medical Billing in the Revenue Cycle Management (RCM) Process?
Medical billing is the administrative process that transforms clinical documentation into billable claims and collected revenue. Within RCM, it operates after patient care is recorded and continues until all payer and patient payments are posted and balances are resolved.
How Does Medical Billing Convert Clinical Services Into Cash Flow?
Billing converts documented services into payment through a standard workflow. Aftercare is delivered, charges are captured, coded with CPT/HCPCS and ICD-10, submitted to the payer, adjudicated under payer rules, and posted as payments or patient balances.
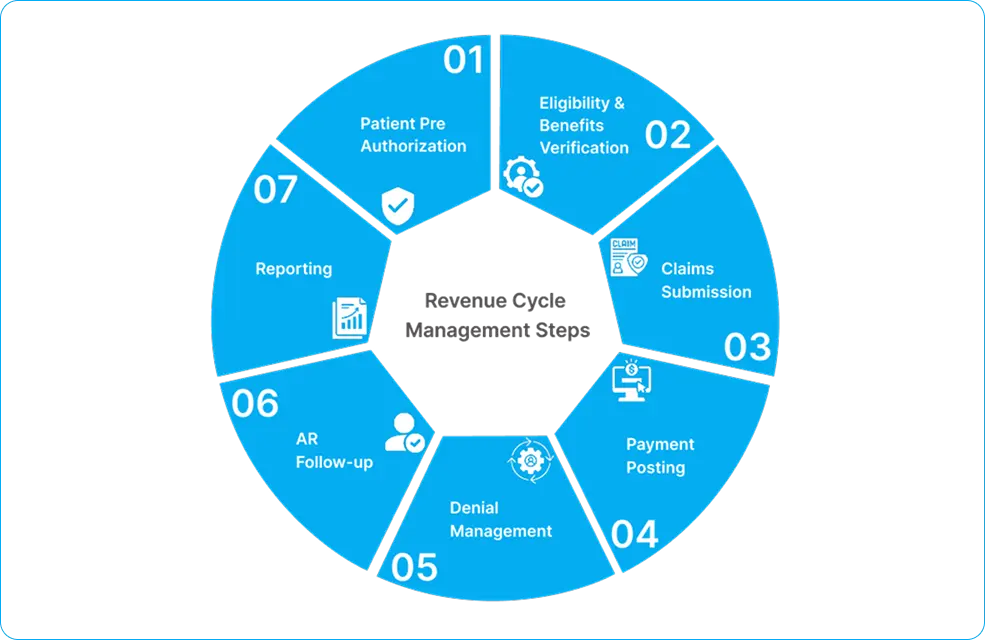
What Is the Claims Lifecycle in Medical Billing?
The claims lifecycle is the path of a claim from creation to closure:
- Charge entry from clinical documentation
- Claim validation and scrubbing
- Electronic submission to the clearinghouse and payer
- Payer review and adjudication
- Payment posting and reconciliation
- Denial handling or appeals if required
- Accounts receivable follow-up until resolution
What Is the Relationship Between Coding, Submission, and Payment?
Coding determines the services reported, submission determines whether the claim reaches the payer correctly, and adjudication determines the final reimbursement. Deficiencies in coding or submission reduce approval rates and extend payment timelines.
Why Does Billing Matter for Financial Sustainability?
Efficient billing stabilizes cash flow by reducing rejections, controlling denials, and speeding up collections. Strong billing lowers A/R days and improves revenue capture, while weak billing increases delays, write-offs, and revenue leakage.
Core Functions of a Medical Billing Workflow
A billing workflow consists of coordinated administrative functions that prevent errors, support compliance, and ensure full reimbursement.
Patient Registration: Collect accurate demographics, insurance identifiers, and coordination-of-benefits data. Errors here lead to failures in eligibility verifications and rejections at the front end.
Insurance Verification: Before billing, confirm the patient has active insurance coverage, benefits, cost-sharing obligations, authorization requirements, and service limits.
Charge Capture: Keep track of all billable services and supplies in clinical documentation to avoid losing revenue.
Medical coding: Use the ICD-10 and CPT codes that show which services were medical necessities and what was done.
Claims Submission: Send verified claims through the clearinghouse as per the required formats for adjudication.
Payment Posting: Use remittance data and contract-based adjustments to get payments from both the payer and the patient.
Accounts Receivable Follow-Up: Check the status of outstanding or underpaid claims, make adjustments, and resubmit them.
Denial Management: Find out why a denial happened, fix the problems, then resubmit or appeal.
Patient Collections: Bill and collect the amount under patient responsibility, such as copays, deductibles, and coinsurance.
What Is In-House Medical Billing?
In-house medical billing means the practice manages the entire billing cycle with its staff. On-site or employed personnel handle coding, claim submission, payment posting, denials, and patient billing.
This model relies on direct employment. The practice hires, trains, and pays the billing team. Payroll, benefits, turnover, and daily operations remain internal responsibilities.
The practice also keeps full control. It sets billing policies, manages workflows, controls access to financial data, and oversees compliance.
Components Required to Operate an In-House Billing System
Running an in-house billing requires staffing capacity, technology infrastructure, and operational oversight to maintain accuracy, compliance, and consistent collections.
Staffing Requirements
Billing Specialists: to handle charge entry, claim submission tasks, payer communications, and basic follow-up activities.
Certified Coders: to assign CPT/HCPCS and ICD-10 codes as per documentation and payer rules to reduce denials and underpayments.
Supervisors: to manage team productivity, denial workflows, performance reporting, and process standardization.
Administrative Support: for registration data accuracy, document collection, patient statements, and coordination between clinical and billing teams.
Technology Infrastructure
Practice Management System: to store patient accounts, claims, payments, adjustments, and aging reports used for A/R control.
EHR Integration: linking clinical documentation to charge capture reduces missing charges and coding gaps.
Clearinghouse Access: to enable electronic claim submission, rejection handling, and payer routing based on payer-specific edits.
Billing Software: to support claim scrubbing, work queues, denial tracking, and reporting functions tied to billing KPIs.
IT Support: to maintain system access, data security, backups, and uptime to protect billing continuity and HIPAA safeguards.
Operational Management
Hiring and Training: for hiring, onboarding, and skills training to maintain coding accuracy and payer rule knowledge.
Performance Monitoring: to track the KPI
Compliance Oversight: to ensure coding accuracy, documentation alignment, HIPAA safeguards, and audit readiness.
Workflow Coordination: the front desk, clinical staff, and billing teams coordinate to prevent registration errors, charge delays, and missing documentation.
What Is Outsourced Medical Billing?
Outsourced medical billing indicates that a healthcare practice contracts a third-party organization, an RCM company, to manage billing. An outside staff takes care of coding, submitting claims, following up, and collecting money.
A contract outlines the services, including the scope, pricing, performance goals, reporting, and compliance duties. Most vendors operate remotely and use secure connections to access the practice’s EHR, practice management system, and clearinghouse.
Scope of Services Provided by Medical Billing Companies
Outsourced billing usually encompasses all RCM tasks, from submitting claims to reimbursement. Depending on the vendor, services may include:
- Manage the entire revenue cycle.
- Specialty coding skills as per payer guidelines and documentation standards.
- Denial management programs to reduce the number of denials and appeals.
- Reporting and analysis of A/R aging, denials, and collection performance.
- Communicating with the payer regarding the status of claims, underpayments, and policy clarification
Service Delivery Models
Medical billing outsourcing is delivered through three common models:
- Full outsourcing: The vendor takes care of most or all of the billing tasks.
- Partial outsourcing: the practice keeps certain jobs in-house and sends others out, such as coding or following up on A/R
- Hybrid arrangements: shared responsibilities where internal staff and the vendor operate connected workflows with defined ownership by function.
Cost Structure: In-House vs Outsourced Medical Billing
In-house billing involves a lot of fixed operational expenses, while in outsourcing many of these costs become one service fee. The comparison below shows how the two models affect finances in different ways.
| Cost Category | In-House Medical Billing | Outsourced Medical Billing |
| Personnel Costs | Salaries, benefits, payroll taxes, overtime | Included in vendor fee |
| Recruitment & Training | Hiring expenses, onboarding, turnover replacement | Vendor manages staffing |
| Management Overhead | Supervisors, performance monitoring | Minimal internal oversight |
| Technology & Software | PM system, billing software, licenses | The vendor provides platforms |
| Hardware & Office Space | Computers, workspace, utilities | Not required |
| IT Support & Security | Maintenance, cybersecurity, backups | Included in service |
| Compliance Risk Costs | Internal audits, penalties, errors | Shared or vendor-managed |
| Pricing Structure | Fixed operating expenses | Variable service fee |
| Upfront Investment | High | Low |
| Scalability Cost | Requires hiring and infrastructure expansion | Scales with contract |
| Hidden Costs | Productivity loss, workflow inefficiencies, revenue leakage | Typically lower due to specialization |
Vendor Pricing Models
| Pricing Model | How It Works |
| Percentage of Collections | The vendor takes a share of collected revenue |
| Cost per Claim | Fixed fee for each submitted claim |
| Flat Monthly Fee | Fixed charge regardless of volume |
| Tiered Pricing | Cost adjusts based on claim volume or services |
ROI Comparison: In-House vs Outsourced Medical Billing
The ROI (Return on Investment) of medical billing depends on its revenue, efficiency, denial prevention, and growth potential. The chart below shows how in-house and outsourced models affect financial performance in key areas.
| Key ROI Driver | In-House Billing | Outsourced Billing |
| Staff Expertise | Depends on internal hiring and training | Access to specialized billing teams |
| Productivity & Capacity | Limited by staff size | Scales with claim volume |
| Error & Denial Rates | Higher risk without dedicated resources | Lower through standardized processes |
| Reimbursement Speed | May slow during workload spikes | Typically faster payment cycles |
| Scalability | Requires hiring and infrastructure | Rapid expansion capability |
| Operational Risk | Staff turnover and knowledge gaps | Vendor responsible for continuity |
| Revenue Optimization | Limited analytics | Data-driven performance improvement |
What Are Key Performance Metrics Used to Compare Billing Models?
These KPIs measure the performance of in-house and outsourced billing in terms of collections, operational speed, claim quality, and financial results. Using the same KPIs for both models, ROI and revenue risk are compared.
| Category | Metric | What It Measures | Why It Matters |
| Collection Metrics | Net Collection Rate (NCR) | Percentage of allowed revenue collected | Indicates how much collectible income is recovered |
| Gross Collection Rate (GCR) | Percentage of total billed charges collected | Shows overall cash recovery from charges | |
| Revenue Capture | Portion of billable services collected | Identifies missed charges and lost revenue | |
| Efficiency Metrics | Days in A/R | Average time to receive payment | Reflects cash flow speed and follow-up effectiveness |
| First-Pass Resolution Rate | Claims paid without rework | Indicates front-end accuracy and clean submissions | |
| Claim Turnaround Time | Time to payer response | Measures processing speed | |
| Quality Metrics | Clean Claim Rate | Claims accepted without rejection | Reflects coding and submission accuracy |
| Denial Rate | Percentage of claims denied | Indicates compliance and documentation issues | |
| Appeal Success Rate | Denials overturned after appeal | Shows effectiveness of denial management | |
| Financial Outcome Indicators | Cash Flow Stability | Consistency of incoming payments | Supports operational planning |
| Profit Margin Impact | Effect on practice profitability | Links billing performance to margins | |
| Revenue Leakage Reduction | Decrease in lost revenue | Measures revenue protection effectiveness |
Control vs Convenience: Operational Trade-Offs
| Factor | In-House Billing | Outsourced Billing |
| Process Control | Full control over workflows and policies | Control delegated to vendor processes |
| Communication Speed | Direct coordination with internal staff | Communication through vendor channels |
| Workflow Flexibility | Easily customized to practice needs | Standardized workflows with limited customization |
| Knowledge Retention | Billing expertise remains internal | Knowledge resides with external team |
| Management Burden | Requires ongoing supervision | Vendor handles staffing and operations |
| Specialized Expertise | Depends on internal hiring | Access to experienced billing specialists |
| Process Standardization | May vary by staff practices | Structured, consistent procedures |
| Accountability | Internal responsibility for outcomes | Contract-based vendor accountability |
Compliance, Security, and Risk Considerations
Medical billing operations must follow the compliance, security, and audit requirements. Risk exposure differs depending on who performs the billing functions and the implemented controls.
| Area | In-House Billing | Outsourced Billing |
| HIPAA Compliance | Practice responsible for policies, training, and safeguards | Shared responsibility; vendor must meet HIPAA requirements |
| Documentation Standards | Internal oversight of clinical documentation quality | Vendor relies on documentation provided by practice |
| Coding Compliance | Depends on internal coder expertise and audits | Specialized coding teams with compliance programs |
| Audit Preparedness | Practice must maintain records and respond to audits | The vendor may assist, but practice remains legally accountable |
| Compliance Expertise | May be limited without dedicated compliance staff | Typically includes experienced compliance resources |
| Audit Exposure | Higher if controls are weak or inconsistent | Risk reduced with structured processes, but not eliminated |
| Data Security Risk | Internal system vulnerabilities | Secure data exchange required across organizations |
| Operational Dependency | Internal staff continuity required | Dependence on vendor performance and availability |
| Contractual Risk | Internal policies govern operations | Service agreements define responsibilities and liabilities |
| Security Controls | Managed internally by practice IT | Vendor must maintain strong technical safeguards |
Scalability and Growth Impact on Practice Operations
Growth leads to more claims, more staff needs, and more complicated operations. The capacity to scale billing services efficiently affects revenue continuity during expansion.
| Growth Factor | In-House Billing | Outsourced Billing |
| Staffing Capacity | Hiring required to handle higher volume | Vendor expands team as needed |
| Hiring Speed | Delays due to recruitment and onboarding | Immediate capacity through existing staff |
| Infrastructure Needs | Additional systems, space, and equipment required | Vendor infrastructure already in place |
| Management Complexity | Increased supervision and coordination | Operational burden handled by vendor |
| Resource Flexibility | Fixed staffing limits adaptability | Resources scale up or down with demand |
| Multi-Location Support | Requires separate coordination per site | Centralized billing across locations |
| Expansion Risk | Revenue disruption during transition periods | Continuity maintained during growth |
What Are The Hidden Factors That Influence Long-Term Financial Outcomes
| Factor | In-House Billing | Outsourced Billing |
| Accountability | Practice responsible for performance and errors | Vendor accountable under contract terms |
| Service Level Agreements (SLAs) | Not applicable internally | Defined performance targets and response times |
| Business Continuity | Disruption risk from staff absence or turnover | Backup teams and continuity plans typically in place |
| Disaster Recovery | Depends on internal IT preparedness | The vendor maintains recovery systems and redundancies |
| Knowledge Dependency | Reliance on key employees | Knowledge distributed across vendor teams |
| Transition Costs | Lower if staying internal | Onboarding, data migration, and process alignment required |
Which Billing Model Is Best for Different Practice Types?
| Practice Type | Key Challenges | More Suitable Model |
| Small or Solo Practices | Limited resources, high cost sensitivity, heavy administrative burden | Outsourced billing often more practical |
| Medium-Sized Practices | Growth management, increasing claim volume, operational balance | Hybrid or outsourced models commonly effective |
| Large or Multi-Specialty Groups | Complex workflows, high volume, scalability needs, strategic control | Either large internal teams or enterprise-level outsourcing |
Decision Framework: How to Choose Between Outsourced and In-House Billing
| Decision Factor | Outsourcing May Be Better When… | In-House May Be Better When… |
| Budget Availability | Limited capital for staffing and systems | Sufficient budget for salaries and infrastructure |
| Claim Volume | Volume fluctuates or is growing | Volume is stable and predictable |
| Specialty Complexity | Requires specialized coding expertise | Services are routine and well-understood |
| Internal Expertise | Limited billing knowledge internally | Experienced billing team already in place |
| Growth Plans | Expansion or new locations planned | Minimal growth expected |
| Desired Control | Operational convenience prioritized | Direct oversight is a priority |
| ROI Potential | Vendor can improve collections and efficiency | Internal team performs at high efficiency |
Scenario-Based Recommendations
| Scenario | Recommended Model |
| Limited budget for staffing and technology | Outsourced billing |
| Rapid growth or expansion planned | Outsourced billing |
| High denial rates or revenue leakage | Outsourced billing |
| Need for specialized coding expertise | Outsourced billing |
| Stable volume with experienced internal team | In-house billing |
| Strong need for direct operational control | In-house billing |
| Existing infrastructure already in place | In-house billing |
Conclusion
There is no single best billing model. The right choice depends on available resources, operational capacity, growth plans, and how much administrative work the practice can manage.
Selecting a model means assessing costs, performance metrics, compliance risks, and scalability needs. The billing structure should match claim volume, specialty complexity, internal expertise, and expansion plans.
The goal is consistent revenue performance: maximizing collections, reducing risk, and maintaining stable cash flow while supporting efficient operations and future growth.
FAQs
What are the benefits of in-house vs. outsourced medical billing?
In-house billing offers direct control and immediate communication, whereas outsourcing provides expertise, scalability, and reduced operational responsibility.
When should a practice outsource medical billing?
Outsourcing is often beneficial when internal expertise is limited, denial rates are high, staffing costs are rising, or expansion is planned.
How long does the medical billing lifecycle typically take?
The lifecycle duration varies depending on the payer and claim complexity, but payment is commonly received within 2–6 weeks when clean electronic claims are submitted.
How long does it take to transition from in-house to outsourced billing?
Transition timelines typically range from several weeks to a few months, depending on data migration, system setup, and workflow alignment.
Will outsourcing billing disrupt ongoing claims processing?
Experienced vendors maintain parallel workflows during onboarding to prevent interruptions in submissions, follow-ups, and reimbursements.
Can a practice outsource only part of its billing functions?
Yes. Hybrid models allow practices to retain selected tasks internally while outsourcing functions such as coding, claim submission, or A/R follow-up.
How are patient billing questions handled when services are outsourced?
Many billing companies provide patient support services or coordinate with practice staff to manage inquiries, statements, and payment issues.
Do outsourced billing companies work with multiple insurance payers?
Most vendors handle a wide range of commercial, Medicare, and Medicaid plans, though coverage depends on the vendor’s experience and contract scope.
How is billing performance monitored after outsourcing?
Vendors typically provide regular reports on collections, denials, A/R status, and other KPIs to track performance and accountability.