Incorrect ICD-10 coding for allergic reactions triggers denials, delayed payments, and avoidable rework, especially when the trigger is unclear or documentation doesn’t support severity. Errors include using unspecified allergy codes, choosing the wrong T-codes vs. Z-codes, and missing key details like initial vs. subsequent encounter, system involved, and presence of anaphylaxis.
This guide explains how to select the correct ICD-10 code for allergic reactions based on trigger, severity, and encounter type, so claims meet medical necessity and payer editing rules on the first submission.
What is an Allergic Reaction?
Allergic reactions are immune-mediated responses to triggers such as food, medications, insect stings, or environmental exposures. Coding accuracy depends on whether documentation supports a true hypersensitivity/allergic reaction versus a non-immune adverse effect or intolerance.
Clinical notes should clearly document “allergic reaction,” and must document 4 elements:
- Trigger (confirmed or suspected)
- Severity (mild reaction vs anaphylaxis)
- Encounter type (A, D, S when required)
- Symptoms and system involvement (skin, airway, GI, cardiovascular)
History of Anaphylaxis vs History of Allergic Reaction ICD-10
Let’s discuss use of the history of codes in allergic reactions.
History of Anaphylaxis ICD-10
Not every patient with a past anaphylactic event is experiencing one today. That’s where history codes come in. A history of anaphylaxis code documents a previous severe allergic reaction that has resolved but remains clinically relevant. Providers often report it when reviewing risk factors, prescribing medications, or assessing future exposure concerns.
History of Allergic Reaction ICD-10
A patient might have a documented allergy history without any current symptoms. History codes help capture those past events in the medical record and alert future providers to potential risks without implying an active allergic condition.
When to Use History Codes vs Active Reaction Codes
The distinction is simple. Historical codes describe something that happened in the past. Active reaction codes describe a condition happening now. A patient with ongoing hives, angioedema, hypersensitivity symptoms, or anaphylaxis requires an active ICD-10 code. A patient whose reaction occurred months or years ago, with no current symptoms or treatment, generally requires a history or allergy status code instead.
Coding vs Clinic Perspective of Allergic Reactions
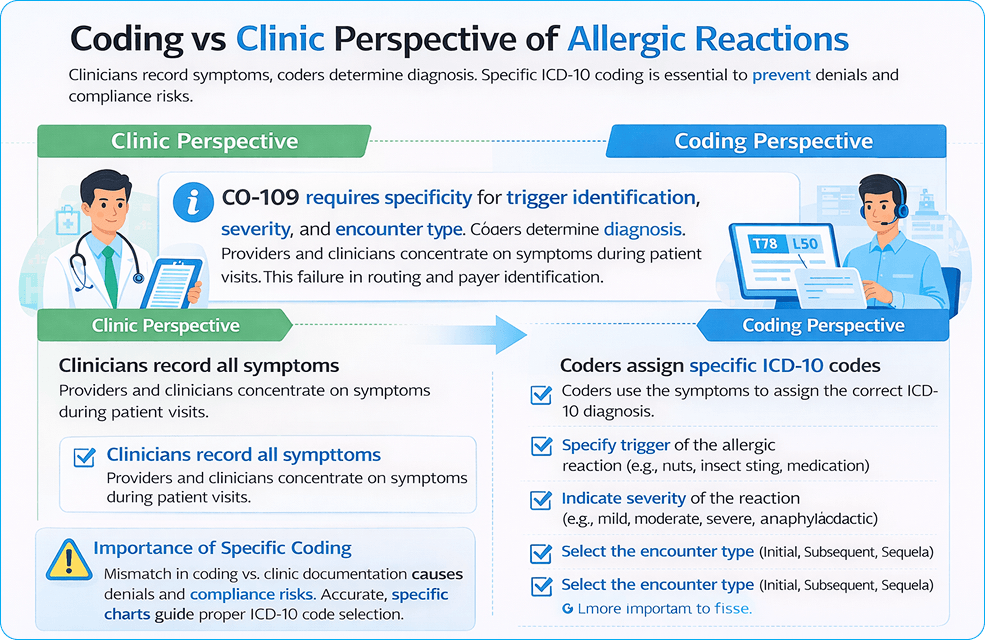
Clinicians document symptoms such as urticaria, angioedema, wheezing, throat tightness, and hypotension. Coders convert that documentation into billable diagnosis codes.
Coding accuracy depends on the same 4 data points:
- Trigger documented in the assessment
- Severity documented in the assessment
- 7th character present for required codes
- Manifestations coded when documented
Coders must identify whether the visit is an initial encounter, a subsequent encounter, or a sequela. Each detail changes code selection and reimbursement impact due to denied claims, payers’ refusal to pay, and compliance risks.
Why is it important to code ICD-10 correctly?
Allergic Reaction ICD-10 coding supports medical necessity and links the diagnosis to the level of service billed. Emergency department and urgent care claims rely on diagnosis specificity for higher-level E/M support. Missing severity and symptom detail weakens the claim when treatment includes epinephrine, IV medications, monitoring, and observation.
Incorrect coding makes payments late, lowers reimbursements, and adds to the workload for administrators. When billing efficiency decreases, healthcare costs increase, and productivity goes down.
ICD-10 Coding Workflow for Allergic Reactions
ICD-10 Coding Workflow for Allergic Reactions
Step 1: Code the Trigger
Identify the allergic reaction trigger (food, drug, insect venom, etc.) to determine the primary code family.
- Food: T78.0
- Drug: T88.6
- Insect: T63.44
Step 2: Code Severity
Determine the severity of the allergic reaction (mild or anaphylaxis).
- Minor reaction: T78.4
- Anaphylaxis: T78.0, T78.2
Step 3: Add the Encounter Type
Ensure the encounter type is documented (Initial, Subsequent, or Sequela).
- Initial encounter: Add code with ‘A’ (e.g., T78.00XA)
- Subsequent encounter: Add code with ‘D’ (e.g., T78.00XD)
- Sequela: Add code with ‘S’ (e.g., T78.00XS)
Follow these 3 simple steps to ensure accurate coding for allergic reactions, preventing claim denials and reducing delays in reimbursements.
Step 1: Code the trigger category
Trigger selection drives the correct code family. Food, drug, insect venom, contact dermatitis, and unspecified reactions do not share the same primary code logic.
Step 2: Code severity
Anaphylaxis requires separate coding from a mild allergic reaction.
Step 3: Add the encounter type when required
T-codes in injury/poisoning sections require the 7th character for a complete code (A, D, S).
ICD-10 Codes for Specific Allergic Reactions
ICD-10 codes show that a diagnosis is medically necessary and help payers decide if they should pay for it. They tell you why a service was needed and how it relates to the patient’s health.
Allergic Reaction to Hair Dye ICD-10
For allergic reactions to hair dye, the most appropriate ICD-10 code is T78.40XA for an unspecified allergic reaction, initial encounter, unless a specific allergen (e.g., para-phenylenediamine) is identified. If the reaction involves a more specific manifestation, such as contact dermatitis, the code L23.9 (Allergic contact dermatitis, unspecified) may also be relevant.
Allergic Hives ICD-10
Hives, or urticaria, are documented under ICD-10 code L50.9 for unspecified urticaria. If the hives are triggered by a specific allergen, such as a drug or food, more specific codes like L50.0 (Acute urticaria) should be used based on clinical details.
ICD-10 Code for Food Allergy Unspecified
For an unspecified food allergy, the correct ICD-10 code is T78.00XA. This code is used when the food trigger is unknown or not documented, and it represents an allergic reaction to food without specification of the type of food.
Allergy to Sulfa Antibiotics ICD-10
The ICD-10 code for a sulfa drug allergy is Z88.1, which is used to document a history of allergy to sulfonamides. If an acute allergic reaction occurs, it should be coded using T88.6XXA for drug-related anaphylaxis.
ICD-10 Code for Itching Unspecified
For unspecified itching (pruritus), the ICD-10 code L29.9 (Pruritus, unspecified) is used when the cause of the itching is not known or documented. If the itching is due to an allergic reaction or skin condition, additional codes like L50.9 (urticaria) may be used, depending on the presentation.
ICD-10 Environmental Allergies Unspecified
Environmental allergies, if unspecified, would typically fall under T78.40XA, for an unspecified allergic reaction, initial encounter, when there is no known environmental trigger. However, for more specific environmental allergens, codes like Z91.81 (History of hay fever) or Z91.89 (Other specified allergy history) could be used in appropriate contexts.
Hypersensitivity Reaction ICD-10
A hypersensitivity reaction, such as an allergic response to a substance, is often coded under T78.4 (Other adverse effects of drugs, medicaments, and biological substances). If the hypersensitivity reaction involves severe symptoms like anaphylaxis, use T78.0XXA (Anaphylactic reaction due to food) or T78.2XXA (Anaphylactic shock, unspecified trigger) as appropriate.
Strawberry Allergy Status ICD-10
The allergy status for strawberries can be documented under Z91.018 (Other food allergy status). This code is used when a patient has a known history of a strawberry allergy, but the allergy is not currently causing an active reaction. For active allergic reactions, use T78.00XA for unspecified food allergies or a more specific code if known.
Hereditary Angioedema ICD-10
Hereditary angioedema is documented with the ICD-10 code D84.1 (Hereditary angioedema). This condition involves recurring episodes of swelling, often triggered by stress, infections, or trauma. It’s a genetic condition distinct from acute allergic reactions and requires specific coding for diagnosis.
Delayed Hypersensitivity Reaction ICD-10
A delayed hypersensitivity reaction, such as a skin reaction to a drug or toxin, is coded under L23.8 (Allergic contact dermatitis due to other agents). For delayed reactions where the cause is identified, the appropriate allergy-related code should be added based on the clinical presentation.
ICD-10 Code for Allergy to Prednisone
For an allergy to prednisone or a corticosteroid, the ICD-10 code T88.7XXA (Unspecified adverse effect of drug) should be used if the patient experiences an adverse reaction. If there is a confirmed allergy (immune response), Z88.8 (Other drug/biologic allergy status) may be applied to indicate a history of drug allergy.
Proper coding explains ER utilization and urgent care utilization. It also supports resource justification when higher-level services are billed.
| Clinical situation | Primary ICD-10-CM code family | Notes |
| Unspecified allergic reaction treated now | T78.40XA | “Allergy, unspecified, initial encounter.” Use when the trigger lacks documentation. |
| Anaphylaxis due to food | T78.00XA (unspecified food) / T78.0-series | Food anaphylaxis belongs to the T78.0 category. |
| Anaphylactic shock, trigger not identified | T78.2XXA | Use when documentation supports anaphylaxis, but the trigger stays undocumented. |
| Angioedema documented | T78.3XXA | Add when angioedema is documented. |
| Urticaria documented | L50.9 (or a more specific L50 code) | Add when hives are documented. |
| Allergic contact dermatitis | L23.9 (or specific L23 code) | Use when contact dermatitis is documented. |
| Anaphylaxis due to the correct drug properly administered | T88.6XXA | Use for drug-related anaphylaxis due to the adverse effect of the correct drug. |
| Anaphylaxis due to vaccination | T80.52XA | Use when a vaccination reaction meets anaphylaxis documentation. |
Drug Allergy Status ICD-10 Codes (Z88 Series)
Drug allergy status codes identify documented medication allergies when no active allergic reaction is present. These codes communicate important safety information, reduce prescribing risks, and help providers avoid medications that previously caused adverse reactions.
Penicillin Allergy Status (Z88.0)
Z88.0 reports a documented history of penicillin allergy. The patient is not experiencing a current reaction, but the allergy remains clinically relevant when selecting antibiotics. Common examples include prior reactions to penicillin, amoxicillin, or ampicillin.
Sulfonamide Allergy Status (Z88.2)
Z88.2 indicates a history of sulfonamide allergy. This code is frequently associated with sulfa drug allergies, including reactions to sulfamethoxazole-containing medications such as Bactrim. It should not be used to report an active allergic event.
Analgesic Allergy Status (Z88.6)
Z88.6 identifies a documented allergy to analgesic medications. Ibuprofen, ketorolac (Toradol), aspirin, and other pain-relieving drugs may fall into this category when supported by the medical record. The code reflects allergy status rather than a current hypersensitivity reaction.
Other Drug Allergy Status (Z88.8)
Some medication allergies do not fit within a more specific Z88 category. Antihistamines such as diphenhydramine (Benadryl), corticosteroids such as prednisone, or less common medication allergies may be captured using Z88.8 when appropriately documented. Careful provider documentation remains essential to support code selection.
Food Allergy Status ICD-10 Codes (Z91.01 Series)
Food allergy status codes document known food allergies when no active allergic reaction is present. They serve as long-term risk indicators in the medical record. Different purpose. Different coding logic. If a patient arrives with hives, angioedema, or anaphylaxis, an active reaction code is required instead.
Peanut Allergy Status ICD-10 (Z91.010)
Z91.010 identifies a documented peanut allergy. A patient may have experienced a prior allergic reaction, severe sensitivity, or even anaphylaxis related to peanut exposure. The code reflects allergy status only, not a current allergic event.
Milk Allergy Status ICD-10 (Z91.011)
Z91.011 reports a history of milk allergy. This differs from lactose intolerance, which involves digestive symptoms rather than an immune-mediated allergic response. Clinical documentation should clearly establish the allergy diagnosis.
Egg Allergy Status ICD-10 (Z91.012)
Z91.012 is assigned when a patient has a documented allergy to eggs or egg-containing products. The code is commonly reported in preventive care, medication reviews, and immunization-related encounters where allergy history affects clinical decisions.
Seafood Allergy Status ICD-10 (Z91.013)
Z91.013 captures a history of seafood allergy. Fish, shellfish, or multiple seafood-related triggers may be involved. Severity varies widely. Some patients report mild reactions. Others carry a significant risk of anaphylaxis after exposure.
Other Food Allergy Status ICD-10 (Z91.018)
Not every food allergy has its own dedicated ICD-10 code. Z91.018 covers other specified food allergies, including reactions to tree nuts, wheat, soy, sesame, fruits, vegetables, or less common dietary triggers. When searching for an ICD-10 code for allergies, this code frequently appears for food allergies that fall outside the more specific Z91.01 categories.
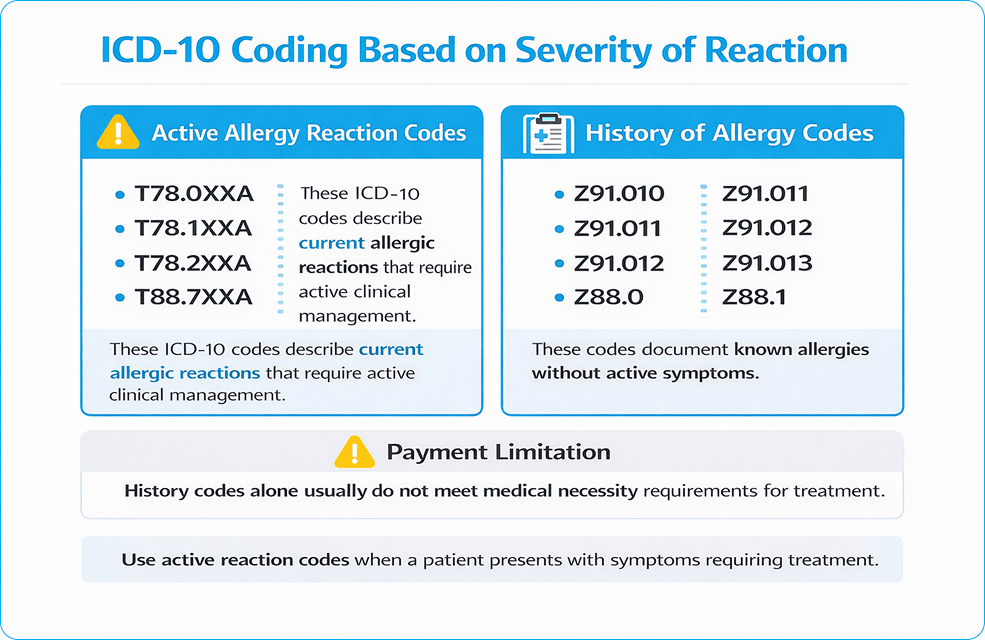
T-Codes vs Z-Codes in Allergy Claims
T-codes represent an active condition treated now. Z-codes represent allergy status or history.
Z-codes that represent history/status (not acute treatment)
Z-codes document allergy history and status, not an active allergic reaction. In allergy billing, these codes fall into three groups: drug allergy status (Z88), food allergy status (Z91.0), and insect allergy status (Z91.03). Use them to support the record when history is relevant, and pair them with T-codes when the visit involves active treatment.
| Allergy history | ICD-10-CM code |
| Peanut allergy status | Z91.010 |
| Milk allergy status | Z91.011 |
| Egg allergy status | Z91.012 |
| Seafood allergy status | Z91.013 |
| Other food allergy status | Z91.018 |
| Penicillin allergy status | Z88.0 |
| Other Antibiotic allergy status | Z88.1 |
| Sulfonamide allergy status | Z88.2 |
| Other anti-infective allergy status | Z88.3 |
| Analgesic allergy status | Z88.6 |
| Other drug/biologic allergy status | Z88.8 |
| Insect allergy status: BEE | Z91.030 |
| Other insect allergy status | Z91.038 |
Claim rule: Z-codes do not support medical necessity for an acute allergic reaction visit when used as the only diagnosis.
T-Codes = Active allergic reaction treated during the visit
- Active Allergic Reaction – T78 Category
| Condition documented | ICD-10-CM code |
| Anaphylactic reaction due to food | T78.0XXA |
| Other adverse food reaction (non-anaphylaxis) | T78.1XXA |
| Anaphylactic shock, unspecified trigger | T78.2XXA |
| Angioneurotic edema (angioedema) | T78.3XXA |
| Allergy, unspecified | T78.40XA |
Use when: The patient is actively treated for an allergic reaction in ED, urgent care, or office.
- Drug-Related Allergic Reactions
| Condition documented | ICD-10-CM code |
| Anaphylaxis due to the correct drug properly administered | T88.6XXA |
| Unspecified adverse effect of the drug | T88.7XXA |
| Generalized skin eruption due to a drug | L27.0 |
| Dermatitis due to drug taken internally | L27.1 |
Use when: Documentation shows immune-mediated drug allergy, rash, or anaphylaxis.
Adverse Drug Reaction vs True Drug Allergy
True drug allergies involve an immune response and hypersensitivity.
Expected side effects and intolerance are not allergies.
- Insect Venom Allergic Reactions (Active Sting)
| Venom source | ICD-10-CM code family |
| Bee venom | T63.44– |
| Wasp venom | T63.46– |
| Hornet venom | T63.45– |
Use when: Patient treated for an active insect sting reaction.
Bee Sting Allergy ICD-10 Codes
Bee sting allergy coding depends on one question: Is the patient having a reaction right now, or is the allergy simply part of their medical history? The answer determines whether an active injury/reaction code or a history code should be reported.
Active Bee Sting Allergic Reaction Coding
An active bee sting allergic reaction requires a code that reflects the current condition being evaluated or treated. Local swelling, urticaria, angioedema, hypersensitivity reactions, and anaphylaxis are coded based on the documented symptoms and severity. The bee sting itself and the resulting allergic response may both affect code selection.
Bee Sting Allergy History Coding (Z91.030)
Z91.030 identifies a personal history of bee sting allergy when no active reaction is present. The patient may have experienced a prior allergic reaction or anaphylactic event after a bee sting, but the condition is not currently being treated. This code serves as a long-term risk indicator and helps alert providers to potential future exposure concerns.
Multiple Drug Allergies ICD-10 Coding
Some patients have a single documented drug allergy. Others have a long list. Penicillin. Sulfonamides. NSAIDs. Contrast agents. The coding challenge is making sure every clinically relevant allergy is captured accurately without overstating the patient’s condition.
Coding Multiple Drug Allergy Status
Multiple drug allergies are typically reported using the appropriate allergy status codes that correspond to each documented medication category. The goal is specificity. A chart that identifies allergies to both penicillin and sulfonamides provides far more clinical value than a vague note stating “multiple drug allergies.”
When Multiple Z88 Codes Can Be Reported
More than one Z88 code may be assigned when a patient has documented allergies involving different drug classes. For example, a patient with a penicillin allergy and a sulfonamide allergy may require both status codes. Each reported code should represent a distinct, documented medication allergy rather than duplicate information.
Documentation Requirements for Multiple Drug Allergies
Details matter. The medical record should identify the specific medication, drug class, or allergy category whenever possible. Providers should clearly distinguish confirmed allergies from side effects, intolerances, or undocumented patient concerns. Strong documentation supports accurate ICD-10 code selection and reduces confusion during future prescribing decisions.
Other ICD-10 codes
Skin/Manifestation Codes (Add when documented)
| Manifestation | ICD-10-CM code |
| Urticaria (hives) | L50.9/L50.8 (or specific L50) |
| Atopic dermatitis (allergic eczema) | L20.9 |
| Allergic contact dermatitis due to plants | L23.7 |
| Allergic contact dermatitis due to metals | L23.0 |
| Allergic contact dermatitis due to chemicals | L23.5 |
| Allergic contact dermatitis | L23.9/ L23.8 (or specific L23) |
| Irritant contact dermatitis | L24.9 |
| Generalized skin eruption due to a drug | L27.0 |
| Dermatitis due to a drug taken internally | L27.1 |
These codes support severity and treatment intensity.
Rule: T-codes explain why treatment was required (E/M, epinephrine, IV meds, monitoring, observation).
Localized Hypersensitivity and Angioedema
| Condition documented | ICD-10-CM code |
| Angioedema (allergic swelling) | T78.3XXA |
| Lip swelling / localized mucosal swelling | K13.0 |
Use rule: Add when swelling is documented as part of the allergic reaction.
Vaccine-Related Allergic Reactions
Vaccine reactions belong to the T80–T88 complication category, not T78.
| Condition documented | ICD-10-CM code |
| Infection following immunization | T88.0XXA |
| Other complications following immunization | T88.1XXA |
| Complication of immunization, unspecified | T88.9XXA |
| Anaphylaxis due to vaccine | T80.52XA |
Hereditary and Immune-Related Allergic Conditions
These are chronic immune disorders, not acute allergic reactions.
| Condition | ICD-10-CM code |
| Hereditary angioedema | D84.1 |
| Immunodeficiency with antibody defects | D80.0, D80.1 |
| Common variable immunodeficiency | D83.0, D83.1 |
| Immune disorder, unspecified | D84.9, D89.9 |
Use rule: These codes apply when the visit addresses the immune disorder itself, not an acute allergy event.
Immunization and status support codes
| Documentation purpose | ICD-10-CM code |
| Immunization was not carried out due to an allergy | Z28.82 |
| Immunization was not carried out due to the patient’s refusal | Z28.21 |
| Under-immunization status | Z28.3 |
| Encounter for immunization | Z23 |
Correct pairing for real claims
| Scenario | Correct coding pattern |
| Patient treated for food-triggered anaphylaxis | T78.0- + (L50.9 if hives documented) + Z91.01x (if known history) |
| Patient treated for bee sting reaction | T63.44- + manifestation code if documented + Z91.030 (history) |
| The patient arrives with an unknown allergic reaction | T78.40XA + manifestation codes |
| Patient follow-up visit with no active reaction | Z91- / Z88- only |
7th Character Rules (A, D, S) for Allergy-Related T-Codes
Many allergy-related T-codes require the 7th character for a complete billable code. Missing the 7th character creates an incomplete code and triggers payer rejection.
| 7th character | Meaning | Typical use |
| A | Initial encounter (active treatment) | ED evaluation, urgent care evaluation, active workup |
| D | Subsequent encounter | Follow-up during the recovery phase |
| S | Sequela | Residual condition linked to a past reaction |
Unspecified Allergic Reaction (T78.40XA)
When the allergen is not known at the time of care, an unspecified allergic reaction is reported. Use T78.40XA in 3 situations:
- The trigger lacks documentation in the assessment
- First-time reaction with no confirmed cause documented
- Emergency presentation where the trigger is unknown at the time of service
When to Code Anaphylaxis as a Separate Issue
Anaphylaxis causes reactions that can kill you. It is important to keep track of multi-system involvement, low blood pressure, and airway compromise.
T78.0XXA, T78.2XXA, T78.6XXA, and T80.52XA are ICD-10 codes for anaphylaxis.
Coding based on severity is very important. Documentation must explain how resources are being used.
How to Document Unspecified Codes
- Record any symptoms like swelling, wheezing, or a rash.
- Please write down any suspected triggers or allergens that you don’t know about.
- Record diagnostic tests, labs, and clinical evaluations.
Why Claims are Denied for Allergic Reactions
Allergy claims are denied when the ICD-10 selection does not match what the chart documents. Payers check specificity, severity, and code structure before payment.
8 denial triggers payers flag:
- Unspecified code used despite available detail
Repeated use of T78.40XA when the trigger, symptoms, or severity are documented. - Wrong primary diagnosis (Z-code misuse)
Using Z88 / Z91 as the primary diagnosis instead of an active reaction code (T78 / T88 / T63). - Missing 7th character on T-codes
Omitting A / D / S creates an incomplete code and triggers rejection. - Severity not reflected in coding
Anaphylaxis, angioedema, urticaria, or respiratory distress documented but not coded. - Manifestations not coded
Hives, dermatitis, swelling, or airway symptoms are present in notes but absent in the diagnosis list. - Diagnosis does not match treatment
Epinephrine, IV antihistamines, steroids, monitoring, or observation without a severity-supported diagnosis. - Trigger not documented
Food, drug, insect sting, or contact exposure not recorded when clinically relevant. - Incomplete clinical notes
Missing symptoms, suspected cause, severity, response to treatment, and encounter type.
How to Prevent Allergy Coding Errors Before Claim Submission
Allergy claim accuracy depends on matching the diagnosis to the documented trigger, severity, and treatment. Denial prevention starts during chart review.
Pre-submission prevention steps (8):
- Select an active reaction code first
Use T78 / T88 / T63 / T80 for visits with active treatment. - Use Z-codes as supporting history only
Add Z88 / Z91 when allergy status matters, not as the primary diagnosis. - Capture the trigger in the assessment
Document food, drug, insect sting, contact exposure, or unknown trigger. - Capture severity in 1 clear line
Document mild reaction, airway symptoms, hypotension, or anaphylaxis. - Add manifestations that appear in the note
Code urticaria, angioedema, dermatitis, respiratory symptoms when documented. - Confirm the 7th character on T-codes
Use A / D / S where required. Claims reject without it. - Match treatment to diagnosis severity
Epinephrine and monitoring require severity documentation. - Avoid repeated unspecified coding patterns
Limit T78.40XA when the chart contains trigger or symptom detail.
Emergency Allergic Care Billing
Looking for professional help with billing for emergency allergic reactions? Our experts provide comprehensive services to manage the complexities of emergency medicine billing, including allergenic emergencies.
For more information, check out our
Emergency Allergic Care Billing
services.
Allergic Reaction ICD-10 Documentation Checklist
Use this checklist during chart review. It reduces denials tied to medical necessity and payer edits.
Required documentation
- The chief complaint states allergic reaction symptoms
- Trigger documented: food, drug, insect sting, contact exposure, unknown
- Onset and timing documented: minutes/hours since exposure
- System involvement documented: skin, airway, GI, cardiovascular
- Key symptoms documented: urticaria, angioedema, wheezing, throat tightness, hypotension
- Severity statement documented: mild reaction vs anaphylaxis
- Treatment provided documented: epinephrine, antihistamine, steroid, IV fluids, oxygen
- Response to treatment documented: improved, persistent symptoms, escalation
- Disposition documented: discharge, observation, transfer, admission
- Encounter type documented when relevant: initial vs follow-up vs sequela (supports A/D/S logic)
Coding checklist
- Primary diagnosis = active reaction code (T78 / T88 / T63 / T80)
- Z-codes added only as history (Z88 / Z91)
- 7th character present for required T-codes (A/D/S)
- Anaphylaxis coded when documented (food/drug/vaccine/unspecified)
- Manifestations coded when documented (urticaria, angioedema, dermatitis, respiratory)
- Trigger category matches documentation (food vs drug vs sting vs contact vs unknown)
- Unspecified code justified when the trigger detail is absent
- Diagnosis supports treatment intensity (epinephrine/monitoring/observation)
Conclusion
Accurate ICD-10 allergy coding comes down to matching the diagnosis to what the chart actually proves: trigger, severity, encounter type, and documented manifestations. Start with an active reaction code (T78/T88/T63/T80), add the 7th character when required, and use Z-codes only as supporting history, not as the primary diagnosis for acute treatment. When documentation supports anaphylaxis, code it explicitly and align the diagnosis with interventions like epinephrine, IV meds, monitoring, and observation. Use the workflow and checklist in this guide before submission to reduce denials, shorten A/R time, and keep allergy claims compliant.
FAQs
What is the ICD-10 code for an allergic reaction?
ICD-10 code T78.40XA is used for an unspecified allergic reaction.
What is the ICD-11 code for an allergic reaction?
KA00 is an ICD-11 code for an allergic reaction.
Which ICD-10 codes are required for food allergies related to anaphylaxis?
T78.00XA code is applicable for unspecified food allergy.
Why do allergy-related medical claims get denied by insurance payers?
Allergy-related medical claims are denied because of incomplete diagnosis, incorrect documentation, or wrong code selection.