Medical billing and medical coding work on three coordinated dimensions: clinical accuracy, payer requirements, and financial performance. Payer requirements are defined by contracts, edits, and coverage policies. Financial performance is visible in accounts receivable, remittance data, and patient balances through medical billing analysis.
When these dimensions are aligned, practices submit claims that move through adjudication with fewer resubmissions of claims and decreased frequency of claim denials.
What is Medical Coding
Medical coding converts clinical documentation into standardized code sets that support uniform reporting, claim submission, and reimbursement processes. Three types of codes are
- CPT code.
- ICD-10-CM system
- HCPCS Level II system
Coders protect payment by ensuring 3 elements:
- What happened (history, exam, assessment, plan, orders, results)
- What gets reported (diagnosis codes, procedure codes, supplies, modifiers, POS)
- What payers accept (coverage rules, bundling edits, unit limits, documentation rules)
What is Medical Billing
Medical billing is the claim and payment side of the revenue management cycle (RCM). Billing converts documented services and assigned codes into transactions that insurers process, pay, deny, or return for correction.
Billing work includes:
- Eligibility checks and benefit details, such as coverage dates, copayments, deductibles, and coinsurance.
- Claim creation and submission through a clearinghouse using standardized electronic transactions.
- Follow-up and resolution through denial management, appeals, and patient statements.
- Payment posting and reconciliation using electronic remittance data, then
- A/R monitoring using aging buckets such as 0–30, 31–60, 61–90, and 91+ days.
HIPAA required national standards for electronic health care transactions to improve administrative efficiency. That requirement is the reason billing teams speak in transaction terms, such as claim submission and remittance advice.
Billing and Coding as One System
Billing and coding are parts of a single chain. A chart that lacks clinical specificity produces coding uncertainty. Coding uncertainty produces claim ambiguity. Claim ambiguity triggers payer edits, requests, denials, or patterns such as upcoding or downcoding that lead to payment disputes.
Data moves through a predictable chain:
- EHR documentation
- Code assignment
- Claim formatting
- Clearinghouse edits
- Payer edits and adjudication
- Remittance and posting
- A/R follow-up and patient billing
Each link depends on the prior link. A clean workflow reduces rework.
HIPAA Checklist for Clean Claims
HIPAA electronic standards define how covered entities exchange claims and related data. That standardization is why the claim journey looks similar across specialties.
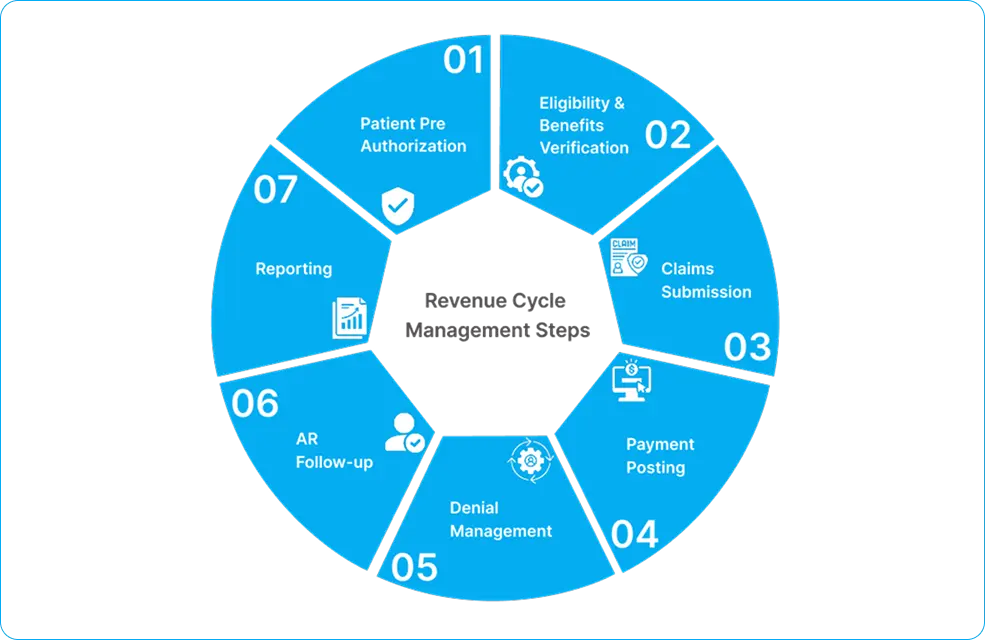
A patient visit becomes a paid claim in 7 operational stages.
1) Eligibility and Benefit Verification
Eligibility answers coverage status. Benefit detail answers financial responsibility. Errors at this stage create patient balance shock and increase self-pay collections work.
Outputs to capture in the patient account:
- Plan name, member ID, group ID
- Copayment amount
- Deductible status and remaining amount
- Coinsurance percentage
- Referral and authorization requirements
2) Referral Management and Prior Authorization
Referral and authorization rules vary by payer and plan type. A missing authorization leads to a denial that cannot be appealed without retro-authorization documentation.
Documentation that reduces disputes:
- Authorization number
- Approved CPT or service categories
- Approved units and date span
- Ordering provider details
3) Provider Documentation and Records Integrity
The HIPAA Privacy Rule applies to covered entities and sets national standards to protect individually identifiable health information. Documentation integrity has two billing outcomes: it supports code selection, and it supports audit defense.
A documentation set that supports payment contains the following:
- Chief complaint and history elements
- Objective findings and test results
- Assessment with diagnosis specificity
- Plan with orders, prescriptions, procedures, and follow-up
- Start and stop times when time drives selection
4) Diagnosis Coding with ICD-10-CM
ICD-10-CM codes classify diagnoses used in patient care reporting and payment logic. Diagnosis coding impacts medical necessity checks, risk models, and coverage rules.
A diagnosis workflow that reduces denials applies 3 checks:
- Specificity check: laterality, acuity, episode of care, complications
- Clinical evidence check: symptoms, results, and assessment alignment
- Linkage check: diagnosis supports the billed service category
5) Procedure and Service Coding with CPT and HCPCS
CPT defines professional services. HCPCS Level II covers products and supplies not in CPT.
Procedure selection becomes stable when the record contains:
- Clear description of what was done
- Site and technique details for procedures
- Units, dosage, and route for drugs and supplies
- Time documentation for time-based services
6) Modifier and POS selection
CMS maintains the Place of Service code set, including telehealth POS 02 and POS 10 definitions. POS influences pricing logic because payers price differently for facility and non-facility settings.
Modifier logic exists to clarify circumstances not visible in base codes. Modifier mistakes trigger bundling conflicts, duplicate logic, or component billing issues.
7) Claim Creation, Scrubbing, Submission, and Adjudication
Claims are transmitted as standardized electronic transactions. The 837 is the claim submission transaction, and the 835 is the remittance advice transaction used for payment explanation and adjustment reporting.
After submission,
- Clearinghouse edits check structure and required fields.
- Payer edits check coverage, bundling, units, frequency, diagnosis linkage, and policy rules.
- The remittance returns payment, denial, or a request path signaled by reason and remark codes.
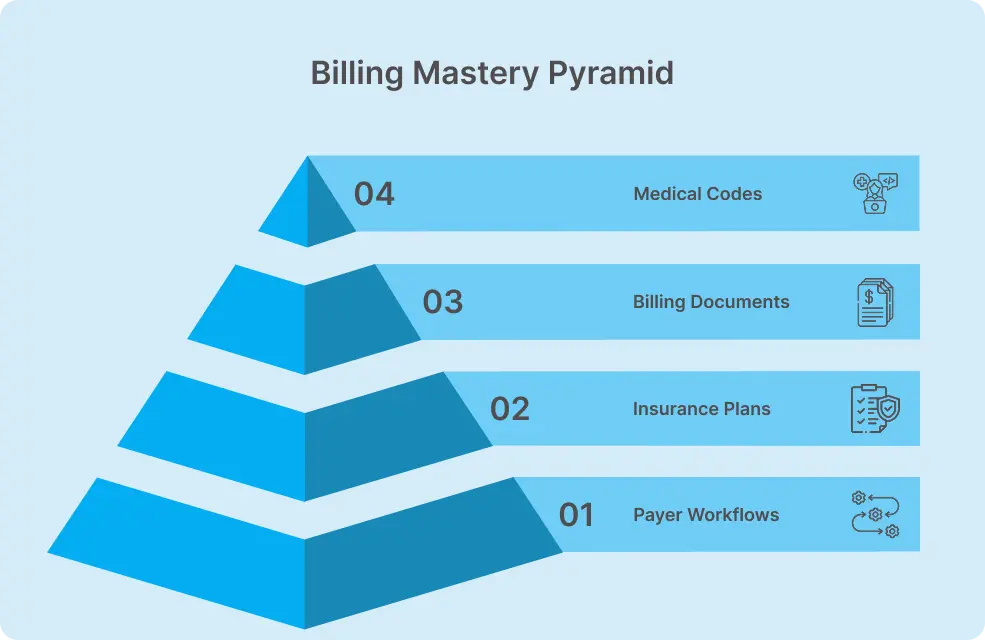
Major Code Sets in Medical Billing

The code set ecosystem is regulated and maintained by defined organizations.
CPT Codes
The American Medical Association describes CPT as a listing of terms and five-digit codes that primarily describe medical services and procedures performed by physicians and other qualified health care professionals.
Operational impact:
- E/M selection determines visit-level reimbursement.
- Procedure coding determines paid line items.
- Category rules determine whether add-on services are separately payable.
ICD-10-CM
The Centers for Disease Control and Prevention describes ICD-10-CM as a system used to code and classify medical diagnoses.
Operational impact:
- Diagnosis drives medical necessity edits.
- Diagnosis specificity reduces “needs more information” requests.
- Diagnosis linkage supports prior authorization validation.
HCPCS Level II:
CMS states that HCPCS Level II identifies products, supplies, and services not included in CPT, such as ambulance services and DMEPOS used outside a physician’s office.
Operational impact:
- Drug J-codes connect to dosage and NDC workflows.
- Supply codes connect to inventory and charge capture.
- Technology services such as remote monitoring depend on HCPCS reporting structures.
In facility and hospital-based billing, payment logic also depends on revenue codes that classify departmental services for institutional claims and affect how services are grouped and priced.
POS Codes
CMS publishes POS Codes that define where services are provided, including telehealth and in-home versus outside the home.
Operational impact:
- POS errors trigger repricing, denials, and recoupments.
- POS consistency improves payer confidence in claims history.
Modifiers: Important Parameter in Claim Accuracy
Correct coding methodologies aim to reduce improper payments from incorrect code combinations. CMS describes the NCCI program as promoting correct coding methodologies and reducing improper coding, with edits that prevent improper payments. That is why modifier use is not “an optional detail.” Modifier use is a payer-facing explanation that determines whether edits allow separate payment.
A modifier workflow that reduces denials follows 4 rules:
- Prove separate work in documentation.
- Match the edit type, such as bundling versus component billing.
- Match the unit structure, such as distinct sessions or anatomical sites.
- Match payer policy because payer-specific requirements override general habits.
High-frequency modifier scenarios:
- Modifier 25: problem-oriented E/M distinct from a preventive service on the same date, supported by separate documentation elements.
- Modifier 26 and TC: split professional interpretation from technical performance in diagnostic testing workflows.
- Modifier 59 and X{EPSU}: distinct procedural service logic used when edits allow separation under defined conditions.
A practice that treats modifiers as “documentation outputs” rather than “billing fixes” produces steadier adjudication.
POS Codes and their Impact on Reimbursement
CMS defines POS 02 as telehealth provided other than in the patient’s home and POS 10 as telehealth provided in the patient’s home. POS influences reimbursement because fee schedules differ across settings.
A POS control process uses 3 checks:
- Scheduling check: visit type and modality captured before arrival or connection
- Clinical check: clinician confirms where the patient received care
- Billing check: POS aligns with claim format and payer telehealth rules
Telehealth errors show up as:
- POS mismatch with modifier expectations
- POS mismatch with payer telehealth coverage windows
- POS mismatch with facility billing rules
Why Claims Get Denied?
CMS describes NCCI edits as preventing improper payments when incorrect code combinations are reported. That same idea extends beyond NCCI. Payers run layered edits that measure internal consistency.
A denial forms when at least one edit condition fails. Denial drivers fall into 5 root cause groups.
1) Identity and eligibility failures
2) Authorization and referral failures
3) Documentation and medical necessity failures
4) Coding and editing failures
5) Format and data failures
A denial management process improves outcomes when it links each denial code to root causes and then fixes the upstream step that produced it.
Pediatric Billing: complex claim patterns
The HIPAA Privacy Rule applies to covered entities and sets national standards for protected health information. Pediatric charts contain immunization details, counseling topics, growth percentiles, and family inputs that raise documentation volume. Pediatric medical billing complexity rises because preventive services and problem-oriented work occur on the same date.
A common pediatric scenario:
- A child arrives for an annual well visit.
- The clinician addresses a separate acute condition, such as otitis media symptoms, asthma flare symptoms, or worsening eczema.
- The chart must separate preventive work from problem-oriented work to support separate reporting.
Operational controls:
- Separate note sections for preventive counseling versus acute assessment
- Diagnosis linkage that connects the acute condition to the problem-oriented service line
- Modifier use supported by documented separate work
Specialty Billing & Coding Rules
The CPT code set describes services performed by qualified health care professionals. Specialty workflows add layers such as diagnostic component splits, global surgical periods, and high-frequency edit pairs.
Specialty billing patterns that trigger denials:
- Diagnostic testing billed without documented interpretation support
- Procedure families billed together without edit-allowed separation conditions
- Units and frequency patterns that exceed payer medical policy thresholds
A specialty control plan uses:
- Specialty templates that capture the minimum required elements
- Edit-driven coding checklists based on frequent denial codes
- Targeted internal audits on the top 20 codes by revenue and the top 20 codes by denial volume
| Specialty | Billing Complexity |
| Cardiology | Diagnostic vs interventional CPTs |
| Radiology | 26/TC split billing |
| Pulmonary | Spirometry Coding & Billing, PFT logic |
| Neurology | EMG/NCS rules |
| GI | Endoscopy bundling |
| Surgery | Global periods |
| Ophthalmology | Eye exam coding |
| Emergency | E/M leveling |
Dental-adjacent specialties, such as orthodontic billing, introduce additional complexity where procedure reporting, documentation standards, and payer coverage rules differ from traditional medical claim patterns.
Documentation: Foundation of Clean Claims
ICD-10-CM is used to code and classify medical diagnoses and is based on defined classification logic. Documentation is the evidence layer that supports that logic.
A “clean documentation” standard includes the following:
- Diagnoses with specificity, not labels alone
- Procedure notes with technique details, not summaries alone
- Orders and results when diagnostics drive decision-making
- Time statements when time-based coding is used
A chart that contains these elements supports claim stability and audit defense.
How to ensure Effeciency of RCM
Revenue cycle management tracks payment from scheduling through reimbursement. A clean claim is the operational outcome of aligned documentation, coding, and claim formatting.
Clean claim drivers:
- Charge capture tied to documented services, supplies, and administered drugs
- Code assignment aligned to guidelines and payer edits
- Claim scrub rules that match payer rejections, not generic checklists
- Posting discipline that ties remittance adjustments to contracts and patient responsibility logic
Performance indicators that show progress:
- First-pass resolution rate
- Denial rate by root-cause group
- Net collection rate
- A/R aging distribution
- Rework minutes per claim
Billing Errors – Revenue Leakage
The False Claims Act imposes treble damages and penalties for knowingly submitting false claims. Revenue leakage is broader than fraud. Leakage comes from routine operational misses.
Leakage patterns:
- Underpayments are missed because the posting team does not compare the paid amounts to the payer’s allowed amount and contract fee schedule expectations.
- Write-offs posted without root cause classification
- Late appeals that miss payer deadlines due to delayed work queues
- Unbilled charges caused by broken interfaces, missing charges, or undocumented supplies
- Patient responsibility drift caused by delayed statements and unresolved coordination of benefits
A leakage control plan connects each adjustment type to a queue owner and a resolution clock.
Compliance Training and Guidelines
The Office of Inspector General explains that establishing and following a compliance program helps physicians submit true and accurate claims and outlines core components for physician compliance programs. The OIG also provides education on fraud and abuse laws, including the Anti-Kickback Statute, and describes penalties and sanctions.
Compliance guardrails that reduce risk:
- Written policies for coding, billing, refunds, and documentation
- Role-based access controls in billing and EHR systems
- Regular internal audits tied to high-risk codes and high-dollar services
- Incident response steps for overpayments and identified errors
- Training calendars tied to annual coding updates and payer policy changes
Stark Law resources are maintained by CMS as part of physician self-referral regulation guidance. Compliance work ties billing accuracy to referral and financial relationship rules.
Role of Medical Billing Services
HIPAA standards and the Privacy Rule shape how billing services handle protected health information and electronic transactions. Outsourcing moves operational work to a business associate relationship that still requires controls, policies, access management, and audit readiness.
Work handled by a billing service:
- Claims submission and rejection correction
- Denial workflows and appeals preparation
- Payment posting and reconciliation
- A/R follow-up and patient statement cycles
- Credentialing and enrollment support as part of payer readiness workflows, including understanding delegated vs non-delegated credentialing responsibilities between practices, billing entities, and payers.
A vendor mention belongs in a neutral “selection criteria” lens.
- Security controls and HIPAA business associate agreement terms
- Proven workflows for edits, denials, and posting discipline
- Reporting that ties denials to root causes and corrective actions
- Specialty experience tied to the practice’s top code families
Conclusion
HIPAA required national standards for electronic transactions, and the Privacy Rule sets standards for protected health information. CPT, ICD-10-CM, HCPCS, POS, and payer edits connect documentation to payment logic.
A practice that treats billing and coding as one system controls denials, stabilizes A/R, and reduces compliance exposure.
FAQs
What is HIPAA, and why does it matter in medical billing?
The Health Insurance Portability and Accountability Act (HIPAA) sets national standards to protect patients’ identifiable health information.
In medical billing, it matters because billing staff routinely access and transmit protected health information during eligibility verification, claim submission, remittance processing, and patient billing—requiring strict compliance to ensure data privacy and security.
How does HIPAA apply to electronic payments and claims?
HIPAA required national standards for electronic transactions. Claims and remittance advice follow standardized transaction formats, including the 837 for claims and the 835 for payment and remittance advice.
Why do billing staff need compliance training?
The OIG states that a compliance program helps physician practices submit true and accurate claims and outlines core compliance components for physician practices. Training operationalizes those components through documentation rules, coding rules, audit routines, and corrective actions.
What role do OIG guidelines play in medical billing?
OIG compliance guidance defines risk areas and provides program structures used by physician practices and billing entities. OIG education on fraud and abuse laws describes prohibited conduct and sanctions.
What is the Stark Law in healthcare billing?
Stark Law is a federal law that prohibits physicians from referring Medicare or Medicaid patients for designated health services (DHS) to an entity with which the physician (or an immediate family member) has a financial relationship, unless a specific regulatory exception applies.
What effect does the Anti-Kickback Statute have on billing?
The Anti-Kickback Statute prohibits offering, paying, or receiving anything of value to influence referrals for services paid by federal healthcare programs.
In billing, claims connected to such prohibited arrangements can trigger audits, repayment demands, penalties, and enforcement actions.
What happens if a practice fails a compliance audit?
When a practice fails a compliance audit, it faces repayment demands, financial penalties, and legal action. Under the False Claims Act, knowingly submitting improper claims can lead to significant fines and enforcement proceedings. Strong documentation and routine internal audits help reduce this risk.
How can practices maintain long-term billing compliance?
Practices maintain billing compliance through written policies, staff training, regular audits, corrective actions, and adherence to Health Insurance Portability and Accountability Act (HIPAA) privacy and transaction standards.