Apply the right codes to upper GI tract treatments for faster claims approval and high reimbursement. CPT 43239 is commonly used for endoscopy, and its incorrect use causes frequent denials. There is a high occurrence of mistakes by the coders in choosing a code that follows diagnostic esophagogastroduodenoscopy (EGD) and the other that uses biopsy.
By mastering CPT 43239, medical coders, billers, and gastroenterologists can minimize audit risk and avoid denials. This guide defines the occasions on which to apply the code and how to prevent the prevalent mistakes of billing.
Understanding EGD With Biopsy
A biopsy EGD is a transoral upper GI endoscopy that is flexible. The endoscope is inserted into the mouth by the physician into the esophagus, stomach, and duodenum.
You use biopsy forceps to get tissue samples. Histopathology testing is done on these tissue samples. A biopsy can help find inflammation, infection, abnormal mucosa, or cancerous changes that cannot be seen just by looking at them.
What Is CPT Code 43239
CPT 43239 represents an esophagogastroduodenoscopy with biopsy. It is used for upper GI endoscopy, with tissue samples used to make a diagnosis. Only in the case of a biopsy conducted in the same session is the code applicable. The cpt 43239 is not defined to be a diagnostic-only code, but the biopsy is the most significant element. In case no tissue is sampled, the code should not be reported.
CPT 43239 is used to find problems in the upper GI tract. The esophagus, stomach, and duodenum are all parts of this. The procedure lets doctors check for conditions that need to be examined under a microscope.
Biopsies are useful for finding out if someone has an inflammatory disease, an infectious disease, or cancer. They also help with staging diseases and making long-term decisions about how to treat gastrointestinal disorders.
What was actually done during the endoscopy will help you choose the right CPT code. You should only choose CPT 43239 when a biopsy is done and recorded. If you use this code incorrectly, you could get downcoding, denials, or audits.
When to Use CPT 43239
When a biopsy is done, CPT 43239 should be reported and clearly written down in the operative note. Tissue sampling must be medically necessary and backed up by clinical symptoms or findings.
The biopsy must be intentional and not incidental. Documentation should explain why the biopsy was required and what abnormal findings prompted tissue collection.
What CPT Code 43239 Covers
CPT 43239 does not include polypectomy or lesion removal. If a polyp or lesion is removed, a different CPT code applies. Bleeding control procedures are also excluded from this code.
Diagnostic EGD without biopsy is reported using CPT 43235. It is wrong to code CPT 43239 without a biopsy.
Practical Use Cases of 43239 CPT Code
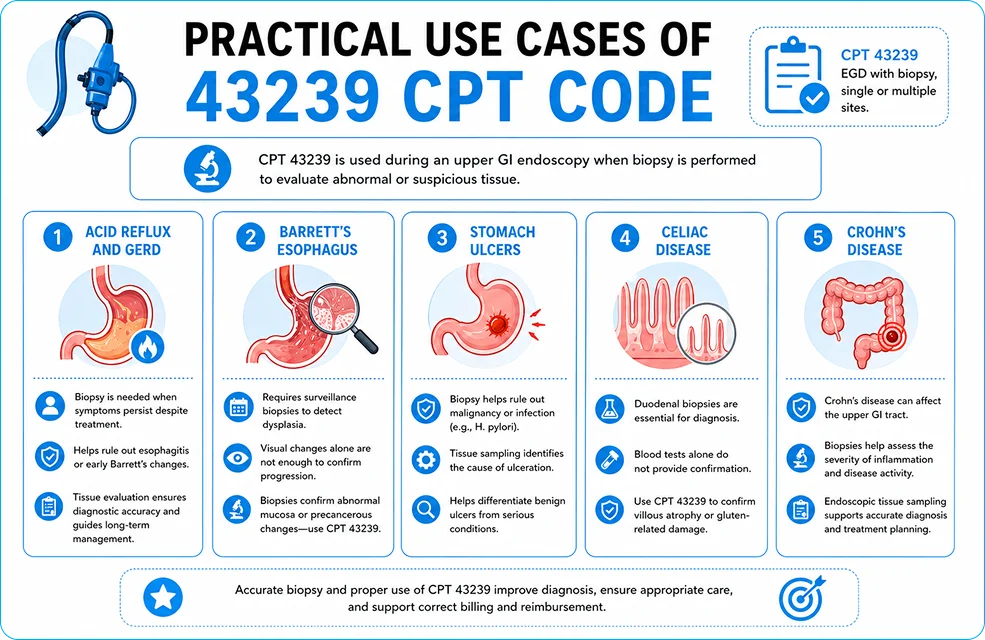
Here are some common situations where you should report CPT 43239.
Acid Reflux and GERD
People with chronic gastroesophageal reflux disease may need a biopsy if their symptoms do not go away even after treatment. Biopsies help rule out esophagitis or early Barrett’s changes.
Tissue evaluation provides diagnostic accuracy and aids in the formulation of long-term management strategies for reflux-related disorders.
Barrett’s esophagus
It usually needs surveillance biopsies to look for dysplasia. Changes in vision alone are not enough to prove that the disease is getting worse.
When biopsies are done to confirm abnormal mucosa or find precancerous changes, CPT 43239 is used.
Stomach Ulcers
A biopsy may be necessary for peptic ulcers to eliminate the possibility of malignancy or infection. Tissue sampling helps find out what is causing the ulceration. Biopsies also help tell the difference between harmless ulcers and more serious problems.
Celiac Disease
Duodenal biopsies are used to diagnose celiac disease. Blood tests alone do not provide confirmation.
If tissue samples are taken to confirm villous atrophy or damage related to gluten, CPT 43239 is the right code to use.
Crohn’s Disease
Crohn’s disease can have an impact on the upper GI tract. Biopsies are useful for figuring out how bad inflammation and disease are. Endoscopic tissue sampling aids in precise diagnosis and treatment formulation.
Other Clinical Signs under 43239 CPT Code
CPT 43239 is also used for anemia that can’t be explained, bleeding in the upper GI tract, and cancer that is suspected. Unusual imaging results may also lead to a biopsy.
These situations necessitate histopathologic validation to inform clinical decisions.
How Payers Evaluate Medical Necessity for CPT 43239
Clinical Indicators That Justify Biopsy During EGD
Payers do not approve CPT 43239 based on procedure alone—they evaluate clinical triggers that justify tissue sampling.
Key indicators include:
- Persistent GERD symptoms despite treatment
- Unexplained iron deficiency anemia
- Upper GI bleeding or melena
- Suspicious mucosal abnormalities on imaging
- Surveillance for premalignant conditions (e.g., Barrett’s esophagus)
Biopsy must be linked to objective findings, not routine exploration. Lack of clear clinical reasoning leads to denials.
Documentation Elements Payers Audit First
During claim review, payers focus on specific documentation checkpoints:
- Explicit mention of biopsy performed
- Exact anatomical site (esophagus, stomach, duodenum)
- Number of samples collected
- Clinical reason linked to ICD-10 diagnosis
- Pathology submission confirmation
Missing any of these elements creates a documentation gap, which directly results in denial under medical necessity rules.
ICD-10 to CPT Alignment Framework
Correct pairing of diagnosis and procedure determines claim acceptance.
| Clinical Condition | ICD-10 Category | Biopsy Justification Strength |
|---|---|---|
| GERD with complications | K21.x | Moderate–High |
| Barrett’s Esophagus | K22.7 | High |
| Gastric Ulcer | K25.x | High |
| Unexplained Anemia | D50.x | Conditional |
| Suspected Malignancy | Cxx.x / R93.x | Very High |
Mismatch between diagnosis and biopsy intent leads to payer rejection or downcoding.
High-Risk Scenarios That Trigger Denials
Certain billing patterns automatically increase audit risk:
- Repeated use of CPT 43239 without variation
- Biopsy performed without documented abnormal findings
- Symptom-only diagnosis without confirmed condition
- Missing linkage between endoscopy findings and pathology
- Overuse of modifiers without justification
These patterns are flagged in payer systems as potential upcoding or non-compliance.
How to Strengthen Claims for First-Pass Approval
To improve clean claim rate, align clinical, coding, and billing layers:
- Document decision-to-biopsy, not just the action
- Ensure ICD-10 reflects confirmed or suspected pathology
- Attach pathology correlation when available
- Avoid generic terms like “rule out condition” without evidence
- Run claims through scrubber + internal audit checklist
Why It’s Important to Code ICD-10 Correctly
There must be a medical reason for doing a biopsy. Just having symptoms may not be enough for the payer to agree.
The ICD-10 code should make it clear why tissue sampling was necessary during the endoscopy.
Common ICD-10 Codes Used with CPT 43239
Common supporting diagnoses consist of GERD, gastritis, gastric ulcers, duodenitis, and inflammatory disorders. People also often use codes for Barrett’s esophagus and possible tumors.
The diagnosis must be consistent with the biopsy justification recorded in the operative note.
Guidelines for Billing CPT 43239
A proper billing workflow makes sure that claims are submitted correctly and payments are made on time. Following billing rules lowers mistakes and makes first-pass acceptance better.
How to Write Documentation
The operative note must make it clear that a biopsy was done. It should say where the tissue sample was taken and why.
Downcoding, or denial, is common when documentation is incomplete or unclear. The biopsy decision must be backed up by ICD-10 codes. The choice of diagnosis should be based on clinical findings, not just symptoms.
When a clear condition is documented, don’t just code the symptoms.
Major Billing Mistakes
Not including biopsy details is a common mistake. Claim failures can also happen when the wrong CPT code and modifier are used.
Before you send it in, make sure to look it over carefully to avoid these problems. The most common reason for denying CPT 43239 claims is a lack of documentation. Patients want to see clear proof that a biopsy was done and was medically necessary. Strong documentation helps with both compliance and getting paid.
What Must Be in an Operative Note
The operative note must say that a biopsy was done. It should say where in the body it is, like the esophagus, stomach, or duodenum.
Clear documentation shows the procedure met CPT requirements.
Biopsy Details That Must Be Included
The number of biopsy samples should be documented. The clinical reason for the biopsy must also be stated.
These details support medical necessity and pathology billing.
Documentation Mistakes to Avoid
Vague procedure notes often result in denials.
Another common problem is not connecting the results to the biopsy.
The paperwork should make it clear why tissue sampling was necessary.
Modifiers Applicable to CPT 43239
Modifiers help explain special circumstances during billing. Incorrect modifier use is a frequent cause of denials.
Understanding when and how to apply modifiers is essential.
Commonly Used Modifiers
Modifier 51 is used for multiple procedures. Modifier 53 applies to discontinued procedures. Modifier 59 identifies distinct procedural services.
Modifiers XE and XP describe separate encounters or providers. Use modifier 22 for more procedural services.
How to Pick the Right Modifier
Before using Modifier 59, make sure that the procedures are really different. Find out if a procedure was stopped or not finished.
Don’t use extra modifiers that might make payers look more closely.
Global vs. Split Billing for CPT Code 43239
The rules for billing depend on where the procedure is done. Knowing about these differences helps avoid mistakes in billing.
There are different rules for getting paid back in each environment. Split billing is used by hospital outpatient departments. The doctor and the facility send separate bills. In this case, the rules for Medicare OPPS often apply.
Billing for an Ambulatory Surgery Center (ASC)
ASC billing follows rules for how much each facility can charge. Rates of pay are different in hospitals. For ASC reimbursement to be correct, coding must be correct.
Endoscopy in the Office
Global billing is common for office-based endoscopy. The doctor sends a bill for both professional and technical parts. The documentation must back up the global service.
Effect of Place of Service
Place of service codes have an effect on how much you get paid and what the payer’s rules are. Choosing the wrong POS can cause payments to be late.
Always check to make sure the billing address is correct.
CPT Code 43239 vs Other EGD Codes
Choosing the wrong EGD code can cause audits and denials. Knowing the differences between codes can help you avoid expensive mistakes.
Each code stands for a different level of service.
CPT 43235 – Diagnostic EGD
If there is no biopsy, use CPT 43235. It only covers looking at it with your eyes.
Using CPT 43239 without a biopsy is incorrect.
CPT 43250 / 43251 – Lesion or Polyp Removal
These codes are used for therapeutic procedures. They include the removal of lesions or polyps.
They are not appropriate for biopsy-only procedures.
CPT 43255 – Bleeding Control
CPT 43255 is reported for active hemorrhage control. It involves therapeutic intervention.
This code should not be confused with biopsy services.
Key Differences & Coding Risks
Using the wrong EGD codes raises the risk of an audit. Good documentation helps you choose the right code. Always write code based on the best service you can give. Billing teams can fix problems faster if they know about common mistakes. Reviewing claims ahead of time increases the chances of success.
Common Denial Reasons for CPT 43239
Payers may state that documentation does not support the biopsy. Bundled service denials are also common.
Messages about modifier inconsistency show that there are coding mistakes.
How to Fix Claims That Were Denied
Look over the paperwork to find any holes. Fix the coding mistakes and send the claim again. Moreover, resubmitting on time leads to better reimbursement results.
CPT 43239 is thought to be sensitive to audits. Using it wrong could lead to payer reviews or compliance audits. A lot of people worry about upcoding from diagnostic EGD. Payers keep a close eye on the reasons for biopsies. Clear records lower the risk of an audit.
Missing pathology links are a cause for concern. Using CPT 43239 over and over again without changing it could also get attention. Auditors look for patterns in the way documents are written.
Regular internal audits of documents help find risks. Ongoing coding education helps people follow the rules. Long-term income is protected by internal controls.
Checklist for CPT Code 43239 Before Submission
A final check before sending in your work lowers the number of mistakes. Checklists help make sure that claims are clean.
These steps save time through efficient denial management.
Checking Before Billing
Make sure the biopsy is written down. Make sure that ICD-10 codes support medical necessity.
Verify clinical alignment.
Coding & Modifier Validation
Confirm modifier necessity. Review bundling rules carefully.
Correct errors before submission.
Final Claim Review
Ensure pathology coordination is complete. Run claims through a scrubber.
Submit only clean claims.
Conclusion
CPT Code 43239 is very important for billing in gastroenterology. For compliance, it is important to keep accurate records, use the right diagnosis codes, and use the right modifiers.
Providers can cut down on denials, avoid audits, and get better reimbursement by following best practices. Proactive billing and thorough documentation protect both the quality of patient care and the money coming in.
Frequently Asked Questions (FAQs)
What is CPT code 43239 used for?
It is used for esophagogastroduodenoscopy. CPT code 43239 is used to describe a procedure in which a healthcare provider performs an esophagogastroduodenoscopy (EGD) with biopsy.
What is the difference between CPT 43235 and 43239?
While CPT 43235 is used for diagnostic endoscopies, CPT 43239 covers procedures involving biopsies.
Does 43239 need a modifier?
Yes, but only if each procedure is performed at a separate anatomical site or for a distinct clinical reason. Modifier 59 may be required, and clear documentation must support the separation.
What are D1 and D2 in endoscopy?
D1 indicates the first part of the duodenum, and D2 indicates the second part of the duodenum.