CPT Code 64483 is reported for lumbar transforaminal epidural steroid injections targeting specific nerve roots. Accurate billing depends on correct modifier use, level selection, and payer-specific requirements. Incorrect reporting creates claim inconsistencies that fail validation and result in denials, bundling conflicts, and reduced reimbursement.
What Is CPT Code 64483 and What Procedure Does It Represent?
CPT 64483 describes a lumbar transforaminal epidural steroid injection (TFESI) performed at a single level. The procedure delivers medication near a spinal nerve root to treat pain caused by nerve compression.
Key characteristics:
Injection performed at the lumbar spine
Targets a specific nerve root
Guided by imaging (fluoroscopy or CT)
Is CPT 64483 a Nerve Block or Epidural Injection?
CPT 64483 is an epidural steroid injection performed via the transforaminal approach.
It is not classified as a facet injection and differs from general nerve blocks due to its targeted delivery near the spinal nerve root.
How Does CPT 64483 Differ From 64484 and Other Injection Codes?
CPT 64483 is used for the first lumbar level, while additional levels and regions require different codes.
Code comparison
Code
Purpose
Region
64483
First lumbar level injection
Lumbar
64484
Each additional level (add-on)
Lumbar
64479
First level injection
Cervical/thoracic
When to use 64483 vs 64484
Use 64483 for the initial level
Use +64484 for each additional level
Do not report 64484 without 64483
Incorrect level selection leads to bundling issues and claim rejection.
What Modifiers Are Required for CPT 64483 Billing?
Modifiers define how the procedure was performed and how it should be interpreted by payers.
Common modifier usage:
RT / LT: identifies side of procedure
50: bilateral procedure (if payer allows)
59 or XS: distinct procedural service when required
Modifier selection by scenario
Scenario
Modifier
Unilateral procedure
RT or LT
Bilateral same-session
50 or RT + LT (payer-specific)
Distinct level or separate encounter
59 or XS
Modifier selection reflects the actual procedure. Incorrect modifier use changes how payers process the claim and results in reduced payment or denial.
Can CPT 64483 Be Billed Bilaterally or at Multiple Levels?
CPT 64483 billing depends on both levels treated and laterality.
Billing scenarios
Scenario
Coding
Single level
64483
Additional levels
64483 + 64484
Bilateral procedure
RT/LT or modifier 50
Overreporting levels or misuse of bilateral modifiers is a common reason for denial.
What Are CPT 64483 Billing Guidelines and Medicare Rules?
Billing follow guidelines set by the Centers for Medicare & Medicaid Services and local coverage determinations (LCDs).
Key requirements:
Medical necessity must be documented
Imaging guidance is required
Diagnosis must support nerve root involvement
LCD and documentation expectations:
Pain must correlate with imaging findings
Conservative treatments should be documented
Procedure frequency meet payer limits
Imaging guidance documented using fluoroscopy or CT. Missing imaging support or a mismatch between imaging and billing levels results in non-covered services and claim denial.
Failure to meet these criteria results in claim rejection during validation.
How Often Can CPT 64483 Be Billed?
Frequency limits are enforced, especially under Medicare.
General frequency guidelines:
Limited to a set number of injections per year
Often restricted per spinal region within a defined time period
Payers evaluate frequency within rolling timeframes and require documented clinical improvement between injections. Repeated procedures without measurable benefit trigger medical necessity denials.
Why frequency violations trigger denials:
Exceeding limits suggests lack of medical necessity
Repeated procedures without improvement raise audit flags
Claims exceeding frequency thresholds are denied automatically.
What Is the Reimbursement and Global Period for CPT 64483?
Reimbursement varies by payer, location, and facility type.
Key factors:
Medicare fee schedule
Geographic adjustments
Facility vs non-facility setting
Global period:
A 0-day global period
Separate evaluation and management services billed when appropriate
Some services are packaged with CPT 64483 depending on payer rules. Incorrect code combinations or bundling conflicts reduce reimbursement and trigger payment adjustments.
What Are the Common CPT 64483 Billing Errors?
Billing errors occur when procedure details do not match coding rules.
Common mistakes:
Incorrect modifier selection
Reporting wrong levels
Exceeding frequency limits
How these errors affect claims
Error Type
What Happens
Impact
Modifier error
Procedure misclassified
Reduced payment or denial
Level error
Incorrect add-on usage
Bundling or rejection
Frequency violation
Exceeds payer limits
Automatic denial
These errors disrupt claim processing and lead to rework and delayed payments.
How Do Payers Validate CPT 64483 Claims?
Payers evaluate CPT 64483 claims as a complete structure, not individual components.
Key validation checks:
Imaging guidance documented
Correct level and add-on usage
Modifier accuracy
How validation works
Validation Layer
What Is Checked
Outcome
Procedure accuracy
Level and region match code
Confirms correct coding
Documentation
Imaging and necessity
Supports claim
Modifiers
Laterality and distinct service
Determines payment
Payers validate CPT 64483 using documentation, imaging evidence, and level-specific coding rules.
Payers cross-verify these elements together. If one component does not match, the entire claim fails validation.
What Are Common Denial Reasons for CPT 64483?
Denials occur when billing does not reflect procedure details or payer rules.
Common denial scenarios
Issue
Cause
Result
Modifier misuse
Incorrect RT/LT or 50
Claim denial
Frequency exceeded
Too many injections
Rejection
Bundling error
Incorrect code combination
Payment reduction
Impact on revenue:
Delayed reimbursement
Increased administrative workload
Multiple resubmissions
When billing logic fails at any stage, it reflects workflow issues that affect revenue cycle performance.
How Can Providers Improve CPT 64483 Billing Accuracy?
Improvement begins before claim submission.
Core process improvements:
Standardize documentation for procedure and imaging
Validate level selection and modifiers
Monitor frequency limits
Tools that improve performance
Control Area
Action
Result
Documentation
Structured templates
Fewer missing details
Coding validation
Pre-submission checks
Higher accuracy
Audits
Regular claim review
Reduced repeat errors
When Should Providers Consider Expert Billing Support?
When these patterns continue, internal processes lack the structure required for accurate billing.
External support helps by:
Aligning claims with payer rules
Reducing denials through structured workflows
Improving reimbursement consistency
Providers facing these challenges benefit from experienced billing teams such as Avenue Billing Services, where procedure accuracy and compliance are managed through specialized systems.
Conclusion
Accurate billing of CPT 64483 depends on how modifier use, level selection, and payer requirements are applied within the claim. When these elements are correct, claims pass validation and support consistent reimbursement. When they are not, inconsistencies trigger denials, rework, and revenue loss.
FAQs
What is CPT 64483 used for?
It is used for lumbar transforaminal epidural steroid injections targeting a nerve root.
What modifier is required for CPT 64483?
RT, LT, or bilateral modifiers are commonly used depending on the procedure.
How often can CPT 64483 be billed?
Frequency depends on payer guidelines, often limited annually or per region.
Can CPT 64483 be billed bilaterally?
Yes, use RT/LT or modifier 50 according to payer rules.
What is the difference between CPT 64483 and 64484?
64483 is for the first level, while 64484 is an add-on for additional levels.
CPT code 99050 represents services delivered outside a provider’s normal operating hours. The code reflects operational requirements for after-hours care. Accurate billing depends on validated service timing, correct code pairing, and alignment with payer policies.
What Is CPT Code 99050 in Medical Billing?
CPT 99050 Definition in the CPT Code Set
CPT code 99050 describes services provided outside regularly scheduled office hours in addition to the primary medical service. The code does not represent a clinical procedure. It reflects the operational condition under which care is delivered.
Unlike procedure-based CPT codes, CPT 99050 is validated based on timing conditions rather than clinical complexity. Eligibility depends on service timing relative to the clinic’s documented operating hours. If the timing requirement is not met, the code is denied regardless of diagnosis or treatment intensity.
Classification as an Add-On CPT Code
CPT 99050 is an add-on code and cannot be billed independently. It must be reported with a primary CPT code, typically an Evaluation and Management (E/M) service.
The primary code represents the medical service provided to the patient. CPT 99050 supplements that service by indicating that the encounter occurred outside standard operating hours. Billing systems validate the presence of a primary code during claim processing. Missing or invalid pairing results in immediate rejection.
Services That Qualify for CPT 99050
CPT 99050 applies for the following services:
evening clinic visits after official closing time
weekend appointments when the clinic is not routinely open
holiday care services requiring staff availability
The clinical nature of the visit does not determine eligibility. Timing relative to clinic hours is the determining factor.
When Can Providers Bill CPT 99050?
Definition of After-Hours Medical Services
After-hours services are defined by the clinic’s official operating schedule. Each practice maintains documented hours that determine when standard services are available.
Payers validate CPT 99050 using objective criteria:
visit timestamp
clinic hours policy
scheduling records
Eligibility is based on documented schedule, not provider judgment or patient urgency. The code is denied if the visit occurs within standard hours.
Clinical Scenarios Where CPT 99050 Applies
CPT 99050 applies where care is delivered outside routine operations. Examples include:
a pediatric patient seen at 7 PM when clinic hours end at 5 PM
a family medicine visit scheduled after normal clinic closure
a weekend walk-in visit when the clinic does not operate regularly
These situations require additional operational support, including staffing and facility access beyond standard hours.
Provider Types That Commonly Use CPT 99050
Primary care physicians, pediatricians, urgent care centers, and internal medicine clinics use CPT 99050 when delivering care beyond routine scheduling window.
When CPT Code 99050 Should Not Be Used
CPT 99050 is reported when timing conditions meet payer-defined after-hours criteria.
Do not use CPT 99050 when:
services occur within routine scheduling window
extended hours are part of routine scheduling (use CPT 99051)
clinic hours are not formally documented
visit timing cannot be verified through records
Payers evaluate eligibility based on documented hours. Misuse commonly occurs when providers confuse unscheduled after-hours services with scheduled extended hours.
CPT Code 99050 Billing Guidelines and Coding Rules
Requirement to Pair CPT 99050 With Primary Service Codes
CPT 99050 requires valid pairing with a primary E/M service. The claim is validated based on:
correct CPT pairing
service timing
payer-specific rules
Primary CPT Code
Service Type
99202–99205
New patient office visit
99211–99215
Established patient visit
The E/M code defines the clinical service. CPT 99050 indicates the timing condition under which that service occurred.
Documentation Requirements for After-Hours Billing
Documentation must include required timing records for after-hours validation
Required records include:
exact visit timestamp
clinic hours policy
provider schedule
Claim Submission Requirements
Billing teams must ensure:
electronic claim submission using ANSI 837 format
claim scrubbing for add-on validation
accurate billing system workflows.
CPT Code 99050 Reimbursement and Payer Policies
Medicare Coverage for CPT 99050
Medicare does not reimburse CPT 99050 separately. The code is bundled into the primary E/M service under the Physician Fee Schedule.
Reimbursement depends on contractual arrangements rather than standard CMS payment structures.
Medicaid Reimbursement Variability
Medicaid coverage varies by state. Programs reimburse CPT 99050 separately, while others exclude or restrict the code.
Providers must verify state-specific policies before billing.
Commercial Insurance Payment Policies
Commercial insurers apply different reimbursement rules:
BCBS may reimburse based on contract terms
UnitedHealthcare often bundles the code
Aetna and Cigna vary by plan
Payment depends on payer agreements and documentation validation.
How CPT 99050 Affects Reimbursement
CPT 99050 adds a supplemental payment when payer policies allow.
Component
Role
E/M Code
Base reimbursement
CPT 99050
Additional operational payment
The code does not increase clinical value. It compensates for operational costs associated with after-hours care.
Typical Reimbursement Range
Reimbursement ranges include:
$10–$50 per visit
higher rates under negotiated contracts
Payment varies significantly by payer and contract structure.
CPT 99050 vs Other After-Hours CPT Codes
CPT Code
Description
Key Difference
99050
After-hours services
Unscheduled outside normal hours
99051
Scheduled extended hours
Routine evening/weekend schedule
99053
Emergency services
Emergency care context
99056
Unusual timing
Rare clinical scenarios
Code selection depends on scheduling structure. Misclassification between CPT 99050 and CPT 99051 is a common cause of claim denial.
Common Billing Errors With CPT Code 99050
Billing During Regular Office Hours
Denials occur when:
visit time falls within posted operating hours
clinic schedules are not clearly defined
extended hours are incorrectly classified as after-hours
Claims fail when service timing does not align with the clinic’s defined operating schedule.
Missing Primary CPT Code
Denials occur when:
no E/M code is submitted
primary CPT code is invalid or unsupported
code pairing fails during claim scrubbing
Claims without proper pairing are rejected at the clearinghouse or payer level.
Payer Policy Violations
Denials occur when:
payer bundles CPT 99050 into the E/M service
contract terms do not allow separate reimbursement
frequency or usage limits are exceeded
Verification of payer policy is required before billing.
Incorrect Documentation of After-Hours Services
Denials occur when:
visit timestamp is missing or inaccurate
clinic hours policy is not documented
records do not align across scheduling and billing systems
Payers require consistent documentation to validate after-hours eligibility.
CPT 99050 Approved vs Denied Scenarios
Scenario
Clinic Hours
Visit Time
Outcome
Reason
Evening visit
9–5
7 PM
Approved
Outside hours
Weekend visit
Mon–Fri
Saturday
Approved
Closed schedule
Extended hours clinic
6–9 PM
7 PM
Denied
Use CPT 99051
Regular hours visit
9–5
3 PM
Denied
Not after-hours
Missing hours policy
Not documented
7 PM
Denied
Cannot validate timing
Documentation Requirements for CPT 99050 Claims
Required Clinical Documentation
Clinical documentation must establish that the service occurred outside standard clinic hours.
Required elements:
visit time (exact timestamp of service)
service type (E/M service provided)
provider availability during the encounter
Documentation must align with scheduling records and reflect the actual time of service delivery.
Administrative Documentation
Administrative records support validation of after-hours billing.
Required records:
clinic hours policy (official operating schedule)
appointment records (scheduled vs actual visit time)
billing notes confirming after-hours designation
Records must support the timing of service delivery relative to the clinic’s operating schedule.
Audit Risk and Compliance
Payers audit CPT 99050 by cross-checking timing data across clinical, scheduling, and billing systems.
Validation includes:
visit timestamp vs clinic hours
consistency across scheduling and billing systems
alignment between documentation and submitted claim
Denials and recoupment occur when
visit time falls within standard hours
clinic hours are not documented
records are inconsistent across systems
Accurate documentation reduces audit risk and supports claim approval.
Revenue Cycle Impact of CPT 99050
Financial Purpose of After-Hours Billing Codes
CPT 99050 exists to recover operational costs associated with delivering care outside standard clinic hours. After-hours services require additional staffing, extended facility usage, and scheduling adjustments that increase practice expenses.
Standard E/M reimbursement does not account for these operational factors. CPT 99050 allows providers to capture incremental value when payer policies permit separate payment.
The financial impact depends on payer contracts. When reimbursed, the code increases total revenue per encounter without altering the clinical service provided.
Operational Benefits for Clinics
CPT 99050 supports both patient access and operational efficiency.
Key benefits include:
extended patient access beyond traditional clinic hours
increased appointment availability without expanding standard schedules
improved utilization of clinical staff and facility resources
additional revenue from after-hours encounters when reimbursed
These benefits allow practices to meet patient demand while maintaining structured scheduling workflows.
Role in Revenue Cycle Management
CPT 99050 integrates into the revenue cycle through multiple validation and processing stages. Accurate use requires coordination between front-desk operations, clinical documentation, coding, and billing systems.
Front-End Scheduling and Eligibility Verification
clinic hours must be defined in scheduling systems
appointment times must be recorded accurately
payer eligibility must be verified before the visit
Incorrect scheduling data leads to downstream billing failures.
Clinical Documentation and Time Validation
visit time must match scheduling records
documentation must confirm after-hours service delivery
provider availability must align with recorded hours
Payers validate CPT 99050 by comparing documentation with clinic hours policy.
Coding and Charge Capture
primary E/M code is assigned based on service level
CPT 99050 is appended when timing criteria are met
coding systems validate add-on code eligibility
Incorrect charge capture leads to claim rejection or denial.
Claim Scrubbing and Submission
billing systems check CPT pairing rules
timestamps are reviewed against clinic hours
payer-specific edits are applied before submission
Claims that fail validation are rejected at the clearinghouse level.
Payer Adjudication and Payment Processing
payer systems verify timing conditions
contracts determine whether CPT 99050 is reimbursed or bundled
allowed amounts are applied based on fee schedules
Denials occur when timing, documentation, or payer rules are not satisfied.
Denial Management and Root Cause Analysis
denied claims are reviewed for timing errors or documentation gaps
corrections are applied to scheduling, coding, or documentation workflows
recurring issues are identified to prevent future denials
This feedback loop improves revenue cycle efficiency and claim acceptance rates.
Which Healthcare Practices Benefit Most From CPT 99050?
Urgent Care Clinics
Urgent care clinics handle high volumes of evening, weekend, and holiday visits. These services often occur outside standard office hours. CPT 99050 applies when care is delivered beyond documented business hours.
Primary Care Practices
Primary care practices use CPT 99050 when providing services outside normal office hours. This includes occasional evening or weekend visits that are not part of routine scheduling.
Pediatric Clinics
Pediatric clinics schedule visits after school hours or during weekends. These encounters qualify for CPT 99050 when they occur outside the documented operating schedule.
Multi-Provider Medical Groups
Multi-provider groups operate with flexible scheduling across multiple providers. CPT 99050 applies when services are delivered outside the group’s standard operating hours.
How Avenue Billing Services Helps Providers Bill CPT 99050 Correctly?
Avenue Billing Services integrates CPT 99050 into end-to-end revenue cycle workflows. This includes
validation of operating schedule,
E/M pairing accuracy,
claim scrubbing against payer rules, and
denial analysis based on timing discrepancies.
These controls reduce rejection rates and improve reimbursement consistency.
Frequently Asked Questions About CPT Code 99050
What does CPT code 99050 mean?
Services provided outside normal office hours.
Can CPT 99050 be billed alone?
No. It must be paired with a primary CPT code.
Does Medicare reimburse CPT 99050?
Medicare does not reimburse CPT 99050 and often bundles it into the primary E/M service.
What is the difference between CPT 99050 and 99051?
99050 applies to unscheduled after-hours services. 99051 applies to scheduled extended hours.
Which providers use CPT 99050?
Primary care physicians, pediatricians, urgent care providers, and internal medicine clinics.
Conclusion
CPT code 99050 allows providers to report services delivered beyond standard operating schedules. Accurate billing depends on validated timing, correct code pairing, and payer compliance. Practices that align documentation with billing rules reduces denials and improves reimbursement outcomes.
From my hands-on experience working with cardiology practices, I’ve seen how often CPT code 78452 becomes a source of confusion for medical billing teams and a loss of revenue for doctors. Many healthcare providers perform the test correctly and document the study, but still face claim rejections. The most common problem is confusion between 78451 and 78452.
In several cases, cardiology practices are losing thousands of dollars simply because the technical and professional components were billed incorrectly, or the ICD-10 code did not fully support medical necessity. These are not rare issues. They happen every week in real medical billing workflows.
To overcome this issue, this blog is written from a billing and compliance perspective, not just a textbook definition. It explains what CPT code 78452 really includes, how payers review it, and how to document and bill it correctly.
What is 78452 CPT Code?
CPT code 78452 is a nuclear medicine procedure used for myocardial perfusion imaging (MPI). It evaluates how well blood flows through the heart muscle using single-photon emission computed tomography (SPECT).
The term “SPECT mult” indicates multiple images obtained during both a rest phase and a stress phase. These image sets allow healthcare providers to compare blood flow under different conditions and identify abnormalities.
In cardiology practice, CPT 78452 is most often used in nuclear cardiology labs and hospital outpatient departments to diagnose coronary artery disease (CAD) and evaluate treatment effectiveness.
The Clinical Purpose of CPT 78452
The clinical purpose of the 78452 CPT code is to identify ischemia, infarction, and other cardiac problems related to decreased myocardial blood flow. It helps determine myocardial viability, detect areas of cardiac injury and also helps the insurance payer to check for approval criteria.
Practical Examples of CPT 78452 Use
CPT 78452 is commonly ordered for:
Unexplained chest pain
Post-revascularization monitoring
Abnormal EKG or stress test findings
Known or suspected coronary artery disease
These indications are routinely reviewed by payers, making diagnosis selection critical for claim approval.
ICD-10 Codes Supporting Medical Necessity for CPT 78452
Correct ICD-10 linkage is one of the most common difficulties for cardiology practices and billing teams. Frequently accepted diagnosis codes include:
R07.2 – Precordial chest pain
I25.10 – Atherosclerotic heart disease
I20.9 – Angina pectoris
R94.31 – Abnormal EKG
Z95.5 – Presence of coronary angioplasty implant
Z86.79 – Personal history of CAD
Incomplete or mismatched diagnosis coding is a leading cause of denials, underpayments, and payer audits for CPT 78452.
Clinical Protocol for CPT 78452
Before the test, patients usually have to fast and have their medications checked. Some medications may be temporarily withheld to ensure accurate results.
Clinical factors like diabetes, high blood pressure, COPD, or arthritis help decide if exercise stress or drug stress is the best choice. Proper preparation helps with both clinical accuracy and the ability to defend documentation during payer review.
Step-by-Step Procedure
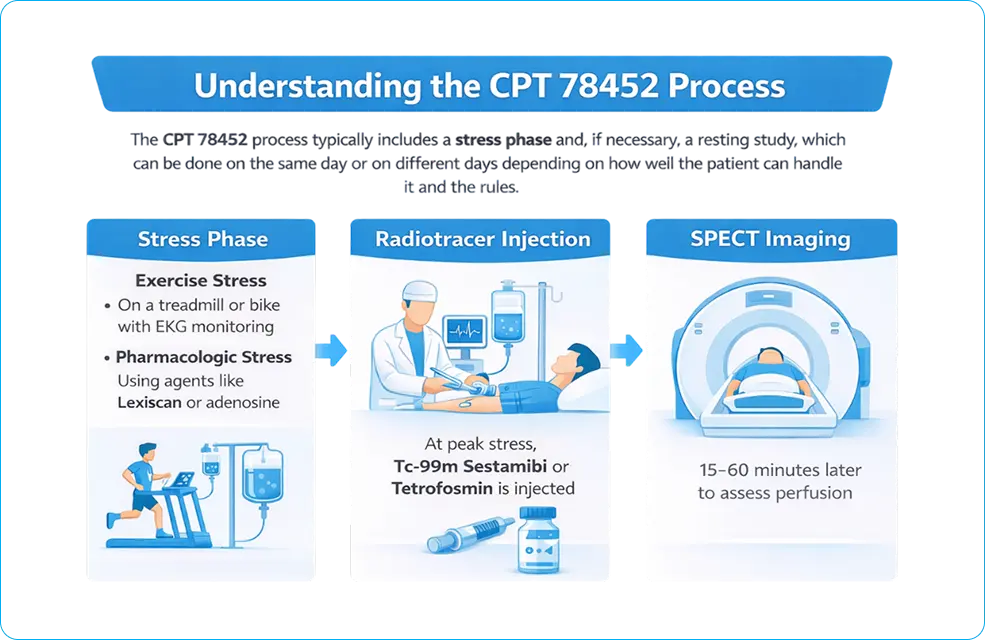
The CPT 78452 process has a stress phase and, if necessary, a resting study. These can happen on the same day or on different days, depending on how well the patient can handle it and the rules.
During the stress phase, myocardial blood flow is increased using:
Exercise stress, like testing on a treadmill or bike, while keeping an eye on the patient’s heart rate with an EKG
Pharmacologic stress, employing agents such as Lexiscan (regadenoson) or adenosine
At the height of stress, a radiotracer like technetium-99m sestamibi or tetrofosmin is injected.
SPECT imaging is done about 15 to 60 minutes after the injection to check perfusion.
SPECT Imaging
SPECT imaging makes 3D pictures of the heart that can be used to measure and describe its condition. These pictures help find problems with blood flow, look at the heart’s structure, and check how well the heart is working overall.
Study at Rest Position
The resting study looks at blood flow in the heart without any stress. CPT 78451 with modifier -52 may apply if only one imaging phase is finished or services are cut back. For compliance, it is important to be able to tell the difference between one study and many studies.
CPT Code 78452 Includes:
Stress and rest imaging phases
Giving radiopharmaceuticals
Getting and processing SPECT images
Seeing blood flow
Interpretation by a doctor and diagnostic reporting
As a whole, these parts make up a single nuclear cardiology service.
78452 vs 78451: Key Differences and Examples
CPT 78452 is for more than one imaging study, while CPT 78451 is only for one imaging study. Some common situations are:
Stress and rest imaging done in one session
Stress imaging is performed first, followed by rest imaging
Incomplete rest imaging is charged as fewer services
Billing mistakes and lost money are common when these codes are used incorrectly.
CPT 78451 has fewer images and is less complicated. CPT 78452 needs more imaging, a more thorough interpretation, and helps with a full cardiac assessment. These differences have a direct impact on reimbursement and audit risk.
Revenue Optimization Strategy for CPT 78452: From Claim to Cash
CPT code 78452 is not just a diagnostic service—it is a high-value revenue driver in cardiology billing. Practices that treat it as a structured financial workflow instead of a single claim achieve higher reimbursement consistency and lower denial rates.
Revenue Leakage Points in 78452 Billing
Most financial loss does not come from outright denials—it comes from silent inefficiencies:
Under-coded services (missing -26 or -TC split billing)
Incorrect ICD-10 sequencing reducing medical necessity strength
Missed drug reimbursement (e.g., J2785 for Lexiscan)
Bundling errors under National Correct Coding Initiative edits
Failure to track payer-specific reimbursement variance
These issues reduce net collection per study even when claims are technically “paid.”
End-to-End Revenue Optimization Framework
A structured approach aligns clinical workflow with payer expectations and financial outcomes:
Stage
Action
Revenue Impact
Pre-Visit
Verify eligibility + authorization
Prevents upfront denial
Clinical
Capture risk factors + prior testing
Strengthens medical necessity
Coding
Align CPT + ICD + modifiers
Improves first-pass rate
Billing
Apply payer-specific rules
Reduces rework
Post-Submission
Track ERA/EOB variance
Identifies underpayment
Audit
Internal compliance review
Prevents recoupments
RPM (Revenue Per Study) Optimization Drivers
Practices that actively monitor these variables outperform others:
Modifier accuracy rate (%)
First-pass claim acceptance rate
Average reimbursement variance by payer
Denial rate for nuclear cardiology services
Turnaround time (DOS → Payment)
Even a 5–8% improvement in clean claim rate for CPT 78452 can translate into thousands of dollars monthly for mid-size cardiology groups.
Payer Contract Leverage Strategy
High-volume imaging codes like 78452 can be used to renegotiate contracts:
Compare allowed amounts across payers
Identify underperforming contracts
Use utilization data as negotiation leverage
Align reimbursement with Centers for Medicare & Medicaid Services benchmarks
Operational Insight
Practices that integrate clinical documentation → coding accuracy → payer logic → financial tracking operate with a closed-loop revenue system.
This eliminates guesswork and transforms CPT 78452 from a high-risk audit code into a predictable revenue stream.
Billing Rules for the 78452 CPT Code
To bill CPT 78452 correctly, you need to pay close attention to payer policies, how to use modifiers, and documentation standards. Mistakes in this area often result in payments being denied or delayed.
Documentation Checklist
ICD-10 clinical indication
Symptoms and risk factors for the patient
Method of stress used
Radiopharmaceutical given
Timing and phases of imaging
Final report and interpretation
How Do Payers Decide to Approve or Deny CPT 78452?
Payers do not evaluate CPT Code 78452 based on the procedure alone. Approval depends on how clinical data supports medical necessity and risk evaluation.
Payer Decision Logic Framework
Payers apply a structured review model across four variables:
Non-specific symptoms (fatigue, general weakness) → denied
Mismatch between diagnosis and test purpose → denial trigger
Example Payer Decision Flow
Clinical Scenario
Payer Outcome
Stable chest pain with risk factors
Approved
Abnormal ECG + suspected ischemia
Approved
Asymptomatic screening
Denied
No prior testing + vague symptoms
Denied
Payers evaluate clinical pathway logic, not just documentation presence. If the test does not logically follow prior findings, the claim fails.
When Does CPT 78452 Require Prior Authorization?
Authorization requirements depend on payer type. The same procedure can be auto-approved, conditionally approved, or strictly denied based on plan rules.
Medicare vs Medicare Advantage
Payer Type
Authorization Requirement
Traditional Medicare
Usually not required
Medicare Advantage
Often required (plan-specific rules apply)
Commercial Payer Authorization Rules
Major payers such as Aetna and Humana apply strict utilization controls.
Authorization is required when:
Test is not preceded by basic diagnostics
Symptoms are non-specific
Frequency exceeds payer thresholds
Required Documentation for Approval
Authorization depends on structured clinical evidence:
Operational Gap: Missing prior test documentation is one of the most common reasons for pre-authorization denial.
CPT 78452 Modifiers
Some common modifiers are;
26: Professional part (interpretation and report)
TC stands for technical component, which includes imaging and equipment.
52: Fewer services
59: Separate procedural service
Does CPT 78452 Need a Modifier?
Modifier use depends on the billing context. Modifiers -26, -TC, -59, -76, -77, -91, or -99 may apply based on repeat services or multiple procedures. Clear documentation is essential to avoid audits. Each modifier must be clearly supported in the medical record.
Related CPT Codes
Related codes include CPT 78451, CPT 78454, and CPT 78480. PET imaging requires different codes and documentation.
Bundling Rules
Services such as stress testing (CPT 93015 or 93017) and pharmacologic agents like J2785 (Lexiscan) must be reviewed carefully to avoid incorrect unbundling.
NCCI Bundling & Compliance Rules
NCCI edits define which services are bundled and which may be reported separately. Failure to follow NCCI rules exposes practices to post-payment audits and recoupments.
What Is Included vs NOT Included in CPT Code 78452
Included services:
Stress and rest SPECT image acquisition
Image processing and reconstruction
Blood flow assessment
Physician interpretation and report
Heart–lung ratio calculation when part of MPI
Not separately reportable:
78580 when performed only as part of MPI
IV access solely for tracer injection
Routine monitoring is inherent to the procedure
Global vs Split Billing
Global billing applies when one entity performs all components
Split billing applies when facilities bill technical services and physicians bill interpretation using -26 and -TC.
Lexiscan (Regadenoson) Coding
Lexiscan (regadenoson) is billed with J2785 at 0.4 mg / 5 mL. Side effects such as flushing or shortness of breath should be documented to support medical need and drug reimbursement.
Real-World Billing & Claim Examples
In office-based cardiology practices, missing modifiers are common. In hospital settings, split-billing errors occur more often. Addressing these issues improves first-pass claim acceptance.
Medicare Reimbursement Policy for CPT 78452
The amount of money Medicare pays back depends on the case, where the person lives, and how well the documentation is done. Medicare Part B pays for drugs, and professional and technical services are paid for separately.
How much will Medicare pay for CPT Code 78452?
The Medicare Physician Fee Schedule (MPFS) and MAC (Medicare Administrative Contractor) specific rules set the payment amount. Rates change from year to year and from place to place.
The quality of the documentation, the rules of the payer, and the medical necessity all affect reimbursement. If you don’t have enough evidence or modifiers, you may not get paid, or your claim may be denied. Many Medicare Advantage plans and private insurers like Humana and Aetna need you to get permission first. If you don’t get approval, your claim could be denied.
Audit Risk Areas for CPT 78452
Audit exposure increases when billing patterns do not match clinical necessity. Payers and auditors target high-cost imaging codes like CPT Code 78452 for compliance review.
High-Risk Audit Triggers
1. Overutilization Without Clinical Indication
Frequent MPI orders without documented symptoms
Screening use without risk stratification
2. Missing Stress Test Documentation
No record of stress method (exercise or pharmacologic)
Incomplete imaging phases (rest vs stress)
3. Incorrect Modifier Usage
Missing or incorrect use of -26 (professional) or -TC (technical)
Global billing without facility alignment
4. Unbundling Violations
Separately billing components included in 78452
Duplicate reporting of related imaging services
Common 78452 Denials and How to Fix Them
Some common reasons for denial are not enough medical evidence, missing modifiers, and mistakes in bundling. Fixing these problems will help you lose less money. Some steps to take to avoid problems are:
checking the diagnosis
accuracy of modifiers
internal audits to keep payments from being late.
Conclusion
After working through countless nuclear stress test claims, payer denials, and delayed payments, one thing is clear: CPT code 78452 is not simple, even though many resources describe it that way.
From real billing experience, most reimbursement issues tied to 78452 are preventable. When documentation, modifier selection, unbundling, and ICD-10 linkage are handled correctly, approval rates improve, and audit risk drops significantly.
Accurate use of CPT code 78452 requires more than knowing the definition. To do this, you need to know what the clinical intent is and what the payer expects. Moreover, the NCCI rules and how Medicare and private insurers really look at these claims are also important. Practices that use this level of accuracy have fewer denials, more reliable payments, and better financial stability.
This guide is based on real-world experience, not theory. It is meant to help cardiology providers, billing teams, and compliance professionals code and bill CPT 78452 with confidence, knowing that their claims are legal, correct, and ready for an audit.
FAQs
Frequently asked questions about the 78452 CPT code use are:
What is CPT code 78452 for?
CPT code 78452 is used for myocardial imaging and PET.
When should 78452 not be billed?
CPT 78452 should not be billed when only a single-phase study is performed (use 78451), when documentation does not support medical necessity, or when services are bundled under National Correct Coding Initiative edits.
Can 78452 be repeated?
CPT 78452 can be repeated only when medically necessary (e.g., new symptoms or inadequate prior study) and must be supported with proper documentation and appropriate modifiers.
What documentation do auditors check?
Auditors verify clinical indication (ICD-10), stress method, radiotracer details, imaging phases (rest + stress), timing, and the final physician interpretation/report aligned with Centers for Medicare & Medicaid Services guidelines.
Is CPT 78452 covered by Medicare?
Yes! It is reimbursed by Medicare.
Is CPT code 78452 a PET scan?
No, CPT 78452 is used for SPECT myocardial perfusion imaging, not PET scan.
What is the difference between 78452 and 78454?
78452 specifies the tomographic (SPECT), including attenuation correction, while 78454 states planar. So the distinction is the type of imaging and the type of camera used.
Can you bill for two CPT codes at the same time?
Yes! It is possible to bill 2 CPT codes at the same time fram,e depending upon the medical conditions found.
Are You Being Underpaid for the 78452 CPT Code?
Underpayments may occur due to contract terms, modifier errors, or payer processing issues.
Medical billing performance relies on a consistent, repeatable discipline: each billed CPT code must correspond to documented clinical services, a covered diagnosis, and payer policies that permit distinct reimbursement. Reviewing CPT guidance from multiple perspectives improves coding accuracy, as CPT definitions, payer edits, and documentation requirements are governed by separate authorities.
CPT Codes: A Reporting Standard for Revenue Cycle
Multiple perspectives matter because CPT rules come from one body, payment rules come from another body, and claim submission standards come from yet another system.
The CPT code set is maintained by the American Medical Association as a standardized language for reporting medical services and procedures. (American Medical Association) Codes route clinical work into billing systems because payers adjudicate claims through standardized procedure reporting.
Professional services typically submit on the CMS-1500 format, while institutional services use the UB-04 format or their electronic equivalents. (CMS) The operational point stays the same across formats: CPT lines represent the “what was done,” while other fields represent the “who, where, why, and under what coverage rules.”
CPT code families support different business purposes:
Category I reports established services and procedures used for routine billing.
Category II supports performance measurement and quality reporting.
Category III tracks emerging technology and new services that still need evidence and adoption.
That structure matters because many payers treat new or emerging services as higher risk for medical review, prior authorization, or coverage limitations.
CPT Payment
Payment starts with RVUs, then the payer policy decides the final amount. Several factors here play a role because a code’s relative value does not guarantee payment, and payment does not guarantee the amount expected.
For Medicare physician services, payment calculation flows through the Physician Fee Schedule, where CPT/HCPCS codes map to RVUs that reflect physician work, practice expense, and malpractice components. CMS explains that fee schedule payment uses RVUs adjusted by geographic indices and multiplied by the fee schedule methodology. (CMS)
Private payers benchmark Medicare values but apply contract terms, bundling rules, and proprietary coverage policies. Denial prevention requires checking both:
Fee schedule logic (what a code is worth)
Coverage logic (whether the code is payable for the diagnosis, place of service, and benefit plan)
CPT Selection
Correct selection matters because coding staff read the chart for proof, auditors read the chart for risk, and payers read the chart for coverage.
CPT selection must be traceable to the clinical record, typically supported by SOAP notes, progress notes, procedure notes, and operative report, and not only in memory. Charge capture becomes accurate when documentation is structured, signed, and linked to the billed date of service.
A denial-prevention template supports three goals:
Prove the service occurred (who performed it, what was performed, time elements when required, findings, and report)
Prove medical necessity (reason for the service and clinical indication)
Prove billing conditions (site of service, laterality, components, and modifier intent)
Medicare documentation reviews frequently find errors tied to missing required elements, incomplete records, and missing authentication. CMS publishes documentation guidance tied to CERT-related errors, which makes “complete notes” a compliance requirement, not an administrative preference. (CMS)
Signature and authentication gaps create preventable denials during medical review. CMS publishes signature requirement guidance for Medicare documentation. (CMS)
ICD-10 Establishes Medical Necessity
The clinician documents the diagnosis, a coder assigns ICD-10, and a payer tests coverage through LCD/NCD rules.
ICD-10-CM diagnosis codes explain why a CPT service is reasonable and necessary. Medicare coverage policy routes through national rules (NCDs) or local rules (LCDs). CMS defines LCDs and describes them as determinations by Medicare contractors regarding whether an item or service is covered within a jurisdiction. (CMS)
Medical necessity denials appear when the diagnosis does not match coverage logic. That mismatch shows up on the remittance as a standardized denial reason code. X12 defines Claim Adjustment Reason Code 50 as non-covered due to lack of medical necessity. (X12)
A repeatable medical necessity workflow reduces coverage denials:
Match the diagnosis to the service using the note’s assessment, impressions, and indications
Check LCD/NCD or payer policy for covered ICD-10 code ranges, frequency limits, and documentation requirements
Document the “why now” using symptoms, abnormal findings, failed conservative care, or risk factors documented in the chart.
Submit the claim with aligned codes so the adjudication engine sees consistency at first pass.
Modifiers Changing the Payment Outcomes
Modifiers are interpreted by NCCI edits, payer bundling logic, and fee schedule component logic.
Modifiers do not “fix” coding. Modifiers explain billing conditions that already exist in the medical record. Denial prevention depends on documenting the condition first, then adding the modifier.
Modifier 25: separate E/M work on the same day as a procedure
Modifier 25 reports a significant, separately identifiable E/M service performed on the same date as another procedure. Medicare guidance describes using modifier 25 for same-day, separately identifiable E/M services and requires documentation that supports the reported E/M criteria. (CMS)
Denial-proof documentation for modifier 25 uses distinct elements:
Separate chief complaints such as cough, rash, and abdominal pain
Separate assessments such as asthma exacerbation, cellulitis, and hypertension
Separate medical decision-making tied to work beyond the procedure note
A denial trigger occurs when the chart merges the E/M and procedure into one undifferentiated paragraph. Payers interpret that structure as a single bundled encounter.
Modifiers 26 and TC
Modifier 26 identifies the professional component, and modifier TC identifies the technical component. CMS guidance describes services that have professional and technical components and explains how modifiers 26 and TC relate to RVU components and billing. (CMS)
Denial prevention for component billing requires documentation that proves:
Who performed the test
Who interpreted the test
Where the equipment and staff costs occurred
Presence of a signed interpretation and report when billing the professional component
Modifier 59 and X{EPSU}: override bundling only when services are distinct
Modifier 59 and the X{EPSU} subset exist to report distinct procedural services that would otherwise be bundled through NCCI procedure-to-procedure edits. CMS publishes specific guidance on proper use and emphasizes that NCCI edits prevent payment for overlapping services except when services are separate and distinct. (CMS)
Documentation must prove separation using facts such as:
Different anatomic sites, such as the left knee, the right shoulder, and the cervical region
Different patient encounters, such as morning clinic, afternoon emergency visit
Different lesions, different incisions, different operative fields
A denial pattern appears when modifier 59 is used without a documented “why the edit does not apply.” CMS guidance supports choosing the more specific X modifier when applicable, rather than defaulting to 59. (CMS)
Modifiers 52 and 53: reduced or discontinued services must match the clinical story
Modifier 52 reports reduced services, while modifier 53 reports discontinued procedures due to circumstances affecting patient well-being. Medicare contractor education and policy materials outline boundaries such as anesthesia timing and the clinical reason for discontinuation. (CGS Medicare)
Denial-proof documentation includes:
The intended procedure and the portion completed
The reason for reduction or discontinuation, such as intolerance, instability, or adverse reaction
The exact stopping point and clinical decision to stop
Modifiers 76, 77, and 91: repeated services require reason, timing, and identity
Repeat-service modifiers exist to distinguish duplicate billing from medically necessary repetition. CMS publishes guidance describing modifiers 76 and 77 as repeat procedures by the same or another physician. (CMS) Medicare guidance on modifier 91 addresses repeat clinical laboratory tests under defined conditions. (Medicare)
Denial-proof documentation for repeated uses:
The clinical reason for repetition, such as worsening symptoms, an inconclusive first test, or treatment response monitoring
Timing, such as same day, same encounter, post-operative period
Ordering provider identity and interpreting provider identity
Global surgery rules change coding logic
Surgeons focus on operative care, coders focus on global periods, and payers focus on what is included in a single payment.
CMS publishes global surgery guidance for Medicare billing, describing reporting requirements and modifier use within global periods. (CMS)
Modifier selection in global periods must be supported by:
Relationship of the subsequent service to the original procedure
Location and setting, such as office, facility, operating room
Timing relative to global days
Surgery denials occur because a separately billed E/M is actually included in the global package, or because a post-op procedure is billed without the correct global modifier logic.
Place of service changes reimbursement
Clinicians document location casually, schedulers assign visit types, and payers price claims based on POS and telehealth rules.
CMS maintains a place of service code set and instructs POS users on professional claims to specify where services were rendered. (CMS)
Telehealth adds a second layer. CMS issued guidance creating POS 10 and revising POS 02 to distinguish telehealth provided in the patient’s home from telehealth provided outside the home. (CMS)
POS mismatch denials occur when the chart location, scheduling location, and submitted POS do not match. Payment changes because facility and non-facility rates differ in many fee schedules.
A POS denial-prevention checkpoint uses three confirmations:
Documented the site in the note
Appointment type in scheduling
POS and modifier rules tied to payer policy
Infographic#02
Why payers deny CPT lines and how remittance codes point to the root cause
Multiple perspectives matter because denials are communicated through standardized code sets, workflow teams work different queues, and appeals succeed only when the record supports the billed line.
Remittance advice uses standardized Claim Adjustment Reason Codes and Remittance Advice Remark Codes. X12 defines CARC 50 as a medical necessity not met. CMS remittance guidance describes reason code 97 as payment included in the allowance for another service or procedure, which aligns with bundling denials. (CMS)
High-frequency denial categories map to operational fixes:
CO-97 included in another service: bundling, missing modifier, unsupported modifier (CMS)
Eligibility and coverage: inactive plan, wrong member ID, coordination of benefits errors
Authorization: missing auth number, expired auth, service outside auth scope
Timely filing: claim submitted outside the payer deadline
EDI and clearinghouse rejection: format, taxonomy, NPI, demographics, code set edits
Denial prevention works better than denial management because the chart and claim are easiest to correct before submission.
Documentation requirements
Compliance teams focus on risk, auditors focus on proof, and clinicians focus on care delivery.
The CERT program reviews a statistically valid sample of Medicare claims to determine whether they were paid properly under Medicare coverage, coding, and payment rules. Documentation is the evidence base for that decision. CMS publishes documentation requirement guidance and error patterns. (CMS)
Documentation elements that support CPT payment across payers include:
Patient identifiers and date of service
Ordering provider and performing provider
Clinical indication and diagnosis support
Procedure details such as technique, findings, complications, and specimens
Interpretation and report for diagnostic services
Authentication, such as signature and credentials, with attestation workflows when required.
Compliance expectations extend beyond Medicare. The HHS Office of Inspector General publishes compliance guidance resources that outline risk areas and compliance program infrastructure.
HIPAA requirements apply to protected health information safeguards. The U.S. Department of Health and Human Services explains that the HIPAA Privacy Rule sets standards to protect medical records and individually identifiable health information, while the Security Rule sets safeguard standards for electronic protected health information. (HHS.gov)
CPT across specialties
CPT codes across specialties differ because payment rules differ by service type, as each specialty has its own high-denial CPT patterns, component billing patterns, and global period patterns.
Radiology workflows frequently depend on modifier 26 and TC, and errors occur when interpretation and technical performance are billed inconsistently. CMS explains component billing and how codes can be professional-only, technical-only, or global. (CMS)
Cardiology coding intersects with global surgery modifiers for staged or related procedures and with component billing for diagnostic tests.
Pulmonary testing involves reduced or discontinued services, particularly when patient tolerance limits test completion. Reduced-service documentation supports correct modifier choice. (CGS Medicare)
Pediatric visits produce frequent modifier 25 denials because preventive services and problem-oriented care occur on the same date. Modifier 25 requires separate documentation for the problem-oriented E/M. (novitas-solutions.com)
GI and surgery trigger NCCI bundling edits because multiple CPT lines occur in the same operative session. NCCI guidance becomes the primary denial-prevention reference. (CMS)
Emergency department coding depends on fast documentation, correct POS logic, and strong medical decision-making capture because claims are submitted before full documentation cleanup.
Clean-claim checklist for CPT
Claim quality depends on front desk data, clinical documentation, coding edits, and payer rules working as one system.
A clean claim checklist works best as a gate, not a suggestion. This 12-point gate prevents the denial categories:
Confirm patient demographics such as name, DOB, policy ID
Confirm eligibility status for the date of service
Confirm authorization status when required
Confirm referring provider and ordering provider data when required
Confirm CPT selection matches the documented service
Confirm ICD-10 selection matches documented assessment and indications
Confirm LCD/NCD or payer policy coverage alignment for diagnosis and frequency
Confirm modifier logic matches documented conditions, not billing preference
Confirm POS matches documented location and payer telehealth rules
Confirm component billing rules for diagnostic services, using 26 or TC only when the chart supports it
Confirm signatures and authentication for reports and orders that require them
Confirm the timely filing window and submission status through the clearinghouse edits
Procedure-based mini guides
Each procedure has a different denial trigger, and denial triggers determine what the note must prove.
These examples show how to link CPT to documentation proof and denial risk. Code descriptions change over time, so internal coding references must be validated against the current CPT resources and payer bulletins.
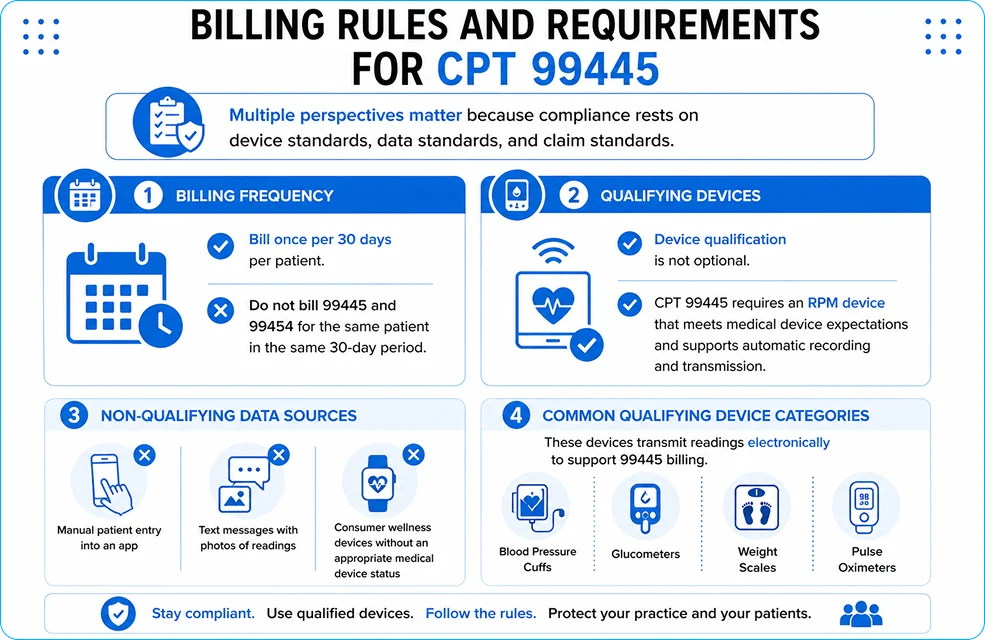
CPT 99445: remote physiologic monitoring device supply for a 2–15 day monitoring threshold in 30 days.
Documentation focus: device supply, data transmission period, patient enrollment, and monitoring dates.
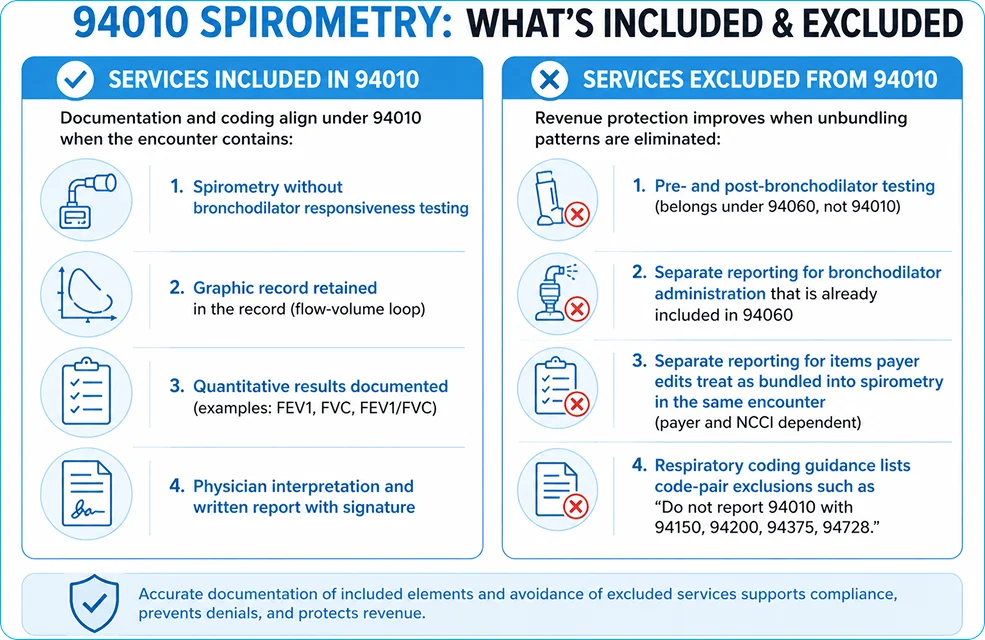
CPT 94010: spirometry testing.
Documentation focus: indication, performance details, results, interpretation, and signed report.
CPT 78452: myocardial perfusion imaging using SPECT in stress contexts.
A procedure guide library becomes more useful when each guide contains three fixed sections:
Coverage rules and frequency limits
Modifier patterns tied to documentation evidence
Top denial codes and appeal evidence checklist
Denial prevention playbook that speeds payment
Multiple perspectives matter because denial prevention is a clinical documentation practice, a coding discipline, and a submission control system.
A denial prevention playbook that works across specialties follows five steps:
Document the indication clearly using symptoms, abnormal findings, and functional limitations
Document the performed service precisely using technique, findings, equipment, laterality, units, and time elements when required.
Document the billing condition using component billing facts, separate E/M facts, and distinct site facts.
Validate coverage before submission using LCD/NCD references and payer medical policy bulletins.
Use remittance analytics to close the loop by mapping CARCs/RARCs to root causes and updating templates and edits.
Conclusion: CPT reimbursement follows the medical record, not the billing software
Multiple perspectives matter because reimbursement is shaped by CPT standards, CMS payment rules, NCCI edits, and payer coverage logic.
CPT coding is maintained by the American Medical Association, and payment logic for Medicare is maintained by the Centers for Medicare & Medicaid Services through fee schedules, coverage policy, and claims processing rules. (American Medical Association) Every payable CPT line needs three alignments: documented service, supported diagnosis, and correct billing conditions such as POS and modifiers.
Denial prevention starts inside the clinical note because payers and auditors validate claims by matching billed lines to documented facts. CERT and medical review programs exist to test whether claims were paid properly under coverage, coding, and payment rules, which makes documentation integrity a revenue-cycle control. (CMS) Compliance guidance resources from the HHS Office of Inspector General reinforce the same operational truth: sustained reimbursement depends on repeatable controls, not ad-hoc fixes after denials. (oig.hhs.gov)
FAQs about CPT coding and denials
What is the difference between ICD-10 and CPT?
ICD-10-CM identifies the patient’s condition, while the CPT Code describes the service performed to treat or evaluate that condition. Payers review both together to confirm medical necessity and coverage. Accurate pairing of diagnosis and procedure prevents coverage-based denials.
How does modifier misuse affect payment?
Modifier misuse triggers bundling and edit failures through NCCI logic and payer rules. CMS publishes guidance on proper modifier 59 and X{EPSU} use, emphasizing separate-and-distinct documentation as the deciding factor.
Why does medical necessity control approval?
Medical necessity is evaluated through diagnosis-to-service coverage rules. CARC 50 is defined by X12 as non-covered due to a lack of medical necessity.
What is a documentation gap in audit terms?
A documentation gap is missing proof required to validate a billed line, such as a missing report, a missing signature, a missing indication, or a missing order. CMS documentation guidance tied to CERT errors highlights these patterns.
How do NCCI edits affect claims?
NCCI edits bundle overlapping services into a single payable line unless documentation supports distinct services. CMS describes this purpose and publishes modifier guidance for appropriate bypass scenarios.
What causes a POS mismatch denial?
A POS mismatch occurs when the submitted POS does not match where the service was rendered. CMS maintains POS code sets and published telehealth POS updates defining POS 02 and POS 10 distinctions. (CMS)
Why do timely filing denials occur?
Timely filing denials occur when the submission exceeds payer deadlines. Operational causes include late charge capture, incomplete documentation, and unresolved eligibility or authorization issues.
How does prior authorization affect CPT payment?
Authorization is a coverage condition in many plans. Missing authorization leads to non-payment even when CPT, ICD-10, and documentation are correct.
Billing teams treat diagnostic laparoscopy as “simple.” Claim outcomes prove the opposite. CPT 49320 sits inside a set of coding rules that reward precision and punish assumptions. A clean claim needs 3 aligned pieces: intent, operative facts, and modifier logic.
CPT content is copyrighted by the AMA. This article paraphrases public-facing descriptors and payer policy guidance rather than reproducing proprietary CPT text.
What CPT 49320 Describes?
CPT 49320 reports diagnostic laparoscopy of the abdomen, peritoneum, and omentum, with or without specimen collection by brushing or washing, and carries the label “separate procedure.”
Clinical work for 49320 centers on inspection. The surgeon introduces a laparoscope through small abdominal incisions and evaluates peritoneal surfaces and abdominal organs. Washings or brushings may occur during the same session and remain included in the code descriptor.
The “separate procedure” label changes how payers treat the code. Separate-procedure services are commonly considered incidental when performed as part of a broader operation in the same anatomic region. The code becomes vulnerable to bundling edits unless documentation supports a distinct service scenario.
Clinical Intent that Supports CPT 49320
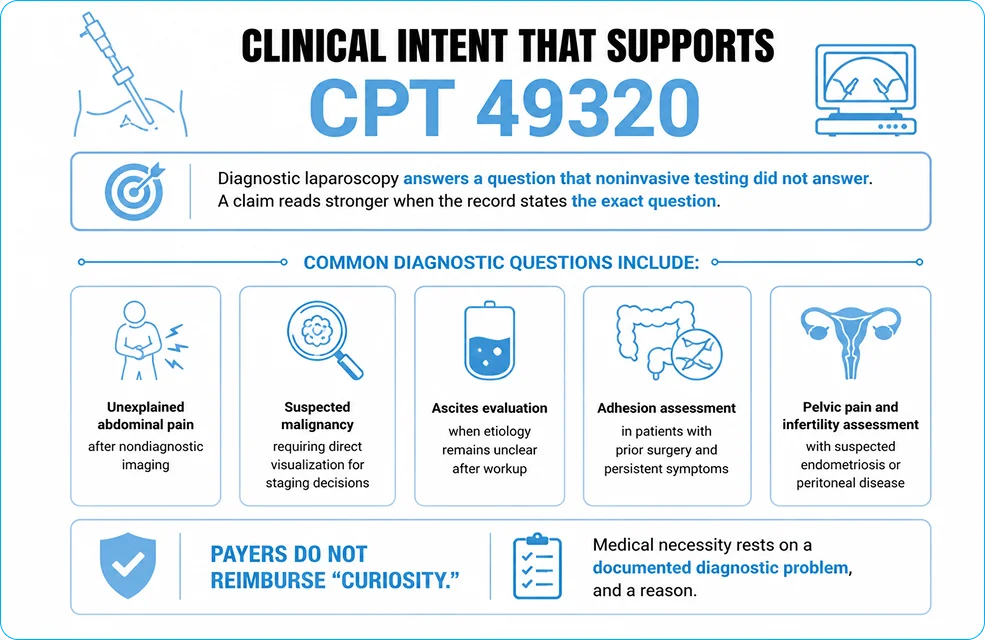
Diagnostic laparoscopy answers a question that noninvasive testing did not answer. A claim reads stronger when the record states the exact question.
Common diagnostic questions include:
Unexplained abdominal pain after nondiagnostic imaging
Suspected malignancy requiring direct visualization for staging decisions
Ascites evaluation when etiology remains unclear after workup
Adhesion assessment in patients with prior surgery and persistent symptoms
Pelvic pain and infertility assessment with suspected endometriosis or peritoneal disease
Payers do not reimburse “curiosity.” Medical necessity rests on a documented diagnostic problem, and a reason imaging or prior testing did not resolve it.
Diagnostic laparoscopy vs therapeutic laparoscopy
CPT 49320 applies to diagnostic-only work. Therapeutic action shifts reporting to a surgical laparoscopy code that describes the performed intervention.
Coding changes at the first therapeutic step, such as:
Biopsy
Aspiration or drainage
Lysis of adhesions
Excision, ablation, or removal of tissue/lesions
Repair of a structure
A frequent error appears in operative reports that describe a diagnostic survey followed by treatment, then attempt to report both the treatment code and 49320. Many payer systems treat diagnostic laparoscopy as bundled into the definitive service in that same session, especially when the diagnostic portion formed the basis for the therapeutic decision. CMS NCCI policy describes this diagnostic-to-therapeutic sequence as a classic bundling scenario.
What is the Staging Laparoscopy CPT Code?
“Separate procedure” status and what bundling means
The CPT label “separate procedure” signals that the service is commonly a component of a more comprehensive service in the same operative field. CPT 49320 includes that label in the descriptor.
Separate reporting becomes reasonable under a narrow set of circumstances, such as:
Different operative sessions on the same date
Different anatomic site/region from the primary procedure
Distinct diagnostic purpose not inherent to the primary procedure
Independent decision-making is documented as distinct from the therapeutic plan
Distinctness must exist in facts, not in narrative tone.
A coding decision path for CPT 49320
Use this 6-step decision path during coding review:
Primary intent stated in the pre-op note as diagnostic evaluation of abdomen/peritoneum/omentum
Operative report documents the survey of the listed inspected structures
No therapeutic service performed beyond brushing/washing
No conversion to another laparoscopic or open procedure that includes exploration as a standard component
No NCCI or payer bundling rule blocks separate payment without an allowed modifier
Claim modifiers match the distinctness scenario, and the record supports the modifier criteria
Step 3 eliminates many disputes. Brushing and washing remain included in 49320 and do not convert the service into a biopsy code.
Modifier strategy that survives payer review
Modifier use should follow payer logic, not habit. CMS states that NCCI-associated modifiers must meet their criteria, and documentation must support the criteria used.
Modifier 59 and the X{EPSU} modifiers (XE, XS, XP, XU)
Modifier 59 indicates a distinct procedural service. CMS recognizes 59 and the more specific subset modifiers:
XE Separate encounter
XS Separate structure
XP Separate practitioner
XU Unusual non-overlapping service
CMS guidance encourages selecting the most specific modifier that describes the distinctness scenario and limiting 59 to cases where no other modifier fits.
Claims involving CPT 49320 most often rely on XS (separate structure) or XE (separate encounter). The record must describe the separate site or the separate encounter clearly.
Distinctness does not come from a different ICD-10 code alone. CMS NCCI policy states that different diagnoses do not unbundle code pairs by themselves.
Modifier 51 for multiple procedures
Modifier 51 signals multiple procedures in the same session. Many payers apply multiple-procedure pricing automatically and do not require 51. Some commercial payers still accept 51 as sequencing support. Payer policy determines whether the modifier belongs on the claim.
A billing rule matters here: modifier 51 does not solve a bundling edit. NCCI distinctness modifiers handle bundling logic.
Modifier 52 for reduced services
Modifier 52 reports a reduced service. CPT 49320 with modifier 52 fits scenarios where the laparoscopic survey could not be completed as intended, yet enough diagnostic work occurred to justify partial reporting.
Limited inspection due to anatomical constraints documented intraoperatively
Operative notes should specify what portion of the diagnostic survey occurred and what blocked completion.
Modifier 53 for discontinued procedure
Modifier 53 applies to a procedure started and stopped due to extenuating circumstances or patient safety concerns. Documentation should include:
Stop time or approximate point of discontinuation
Clinical trigger, such as hemodynamic instability
Services performed up to discontinuation
Assistant surgeon modifiers (80, 81, 82) and modifier AS
Assistant surgeon reporting depends on payer credentialing rules and medical necessity. Claims need documentation that supports the assistant’s role. Modifier AS applies to qualified non-physician assistants when permitted by the payer.
Documentation Standards that Reduce Denials in CPT 49320 Billing
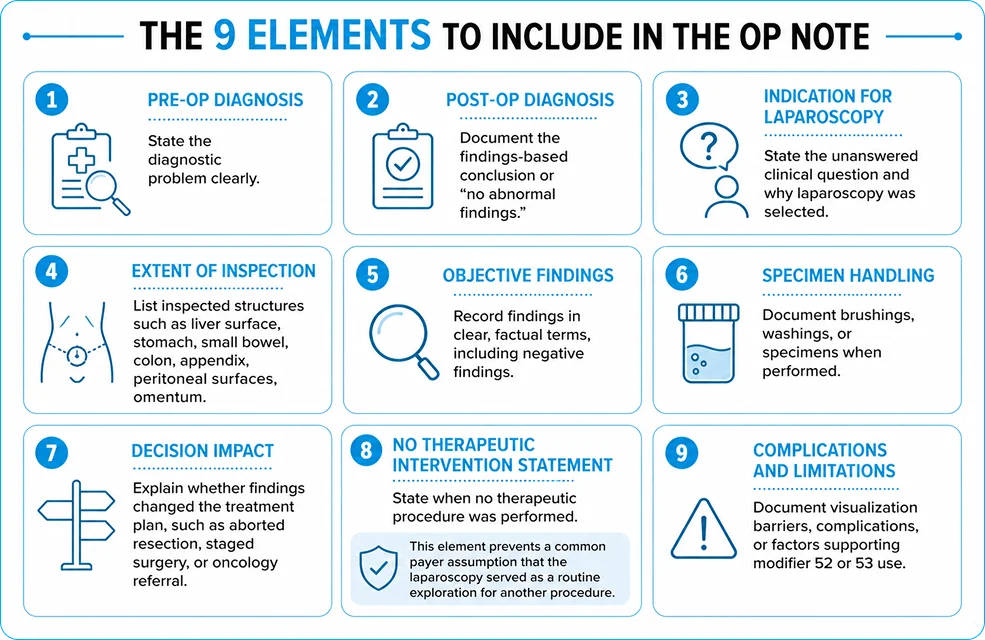
A payer cannot “see” your intent. The operative report supplies proof. A denial-proof report for CPT 49320 contains 9 elements.
The 9 elements to include in the op note
Pre-op diagnosis stated as the diagnostic problem
Post-op diagnosis stated as findings-based conclusion or “no abnormal findings.”
Indication stating the unanswered clinical question and why laparoscopy was selected
Extent of inspection listing surveyed structures (examples: liver surface, stomach, small bowel, colon, appendix, peritoneal surfaces, omentum)
Findings stated in objective terms, including negative findings
Specimen handling, documenting brushings/washings when performed
Decision impact stating whether findings changed the plan (examples: aborted planned resection, staged later surgery, referred to oncology)
No therapeutic intervention statement when appropriate
Complications and limitations documenting barriers to visualization for 52/53 use
Element 8 prevents a common payer assumption that the laparoscopy served as a routine exploration for another procedure.
Specimen collection: brushing and washing
Brushing and washing are included in CPT 49320 per the descriptor language. Separate billing for that collection invites overcoding denials.
Pathology billing follows its own rules. A cytology or pathology interpretation code may apply for the lab component under the appropriate billing entity and payer policy, yet the collection remains included in 49320.
Medicare reimbursement: how payment gets set
Medicare physician payment uses the Physician Fee Schedule (PFS). CMS publishes annual updates and makes pricing, RVUs, and payment indicators available through the PFS Look-Up Tool.
Two Medicare concepts shape expected reimbursement workflow:
Facility vs non-facility payment
Medicare often pays different amounts for the same CPT code based on place of service. A hospital outpatient department or ASC counts as a facility. A physician’s office setting counts as a non-facility. Diagnostic laparoscopy typically occurs in a facility setting, so facility pricing often applies.
CMS finalized multiple PFS policy changes for CY 2026, and the PFS final rule summary remains the authoritative source for current-year policy framing.
Global surgical package and global days
Global periods affect post-op visit billing and related claim edits. Public payer resources list CPT 49320 with a 10-day global period in common global-day references.
Medicare global surgery policy states that post-operative visits within the global period are packaged into payment for many procedures.
NCCI, MACs, and why local rules still matter
NCCI edits influence whether Medicare pays two procedure codes together on the same date of service. CMS publishes NCCI policy manuals and modifier guidance that MAC systems use during claims processing.
Medicare Administrative Contractors (MACs) administer claims and apply national policy plus local coverage rules. Local Coverage Determinations (LCDs) may shape documentation expectations for certain indications or associated testing.
A practical takeaway: coding logic should align with NCCI policy first, then payer contracts, then local MAC articles.
The 7 most common CPT 49320 denial triggers
Diagnostic survey performed before a therapeutic procedure in the same session, then billed separately
Modifier 59 appended without a distinctness fact pattern supported in the op note
The separate-procedure label was ignored and billed alongside a more comprehensive abdominal/pelvic surgery with no separate indication
Operative report lacks inspected-structure detail, so the payer treats the service as a routine look
Specimen collection is billed separately, even though 49320 includes washing/brushing collection
Incorrect discontinued/reduced modifier selection with no stop reason or incomplete service description
Diagnosis mismatch between the clinical question and the submitted ICD-10 code set, weakening medical necessity
CMS NCCI policy highlights the misuse of modifier 59 and states that documentation must meet the criteria for any NCCI-associated modifier used.
CPT 49320 compared with nearby codes
CPT 49320 vs CPT 49321 (biopsy)
CPT 49321 applies to laparoscopy with biopsy. Tissue sampling changes the procedure category from diagnostic survey to surgical laparoscopy with biopsy. Teams should code the biopsy service when performed, rather than reporting 49320.
CPT 49320 vs CPT 49322 (aspiration)
CPT 49322 describes aspiration of a cavity or cyst by laparoscopy. Fluid aspiration moves the service into a therapeutic intervention code set.
CPT 49320 vs CPT 49000 (open exploration)
CPT 49000 describes open exploratory surgery of the abdomen. CPT 49320 describes laparoscopic exploration and diagnostic visualization. The approach and typical recovery differ, and the code families differ accordingly.
ICD-10 linkage: diagnosis selection that supports medical necessity
ICD-10 codes tied to 49320 should reflect the diagnostic problem. Common categories include:
Abdominal pain syndromes
Ascites and peritoneal fluid disorders
Suspected intra-abdominal malignancy or metastatic disease workup
Peritoneal disorders
Infertility-related pelvic pain conditions under payer policy
A defensible claim shows alignment between:
Ordering workup and imaging results
Pre-op diagnosis
Indication statement
Procedure performed
Findings and post-op diagnosis
Real-world billing scenarios
Scenario 1: Diagnostic-only laparoscopy, no additional procedure
Clinical facts: Persistent abdominal pain, imaging nondiagnostic. Surgeon performs a full diagnostic survey. No biopsy, no lysis, no aspiration.
Coding outcome: CPT 49320 alone. No modifier required under standard circumstances.
Documentation cue: A single sentence stating “No therapeutic intervention performed” reduces payer assumptions.
Scenario 2: Diagnostic survey leads directly to treatment in the same session
Clinical facts: The surgeon begins with a diagnostic survey. Findings show endometriosis lesions. Surgeon excises or ablates lesions during the same operative session.
Coding outcome: Report the definitive therapeutic laparoscopy code. Diagnostic laparoscopy becomes bundled in many payer systems, especially when the diagnostic work served as the basis for the treatment decision. CMS NCCI policy describes this diagnostic-to-therapeutic pathway as a common bundling concept.
Documentation cue: The op note should still document the diagnostic survey, yet billing should focus on the performed therapeutic service.
Scenario 3: Discontinued diagnostic laparoscopy due to patient instability
Clinical facts: Procedure begins. Hemodynamic instability develops after insufflation. Surgeon stops the procedure.
Coding outcome: CPT 49320-53 with a clearly documented reason for discontinuation and what was completed before stopping.
Documentation cue: Include objective vitals trend or anesthesiology note reference, and the exact point of termination.
A claim-ready checklist for CPT 49320
Use this checklist before claim submission:
Indication supports medical necessity and matches ICD-10
Op note lists inspected structures and findings
Statement clarifies diagnostic-only intent when no therapeutic work occurred
Washing/brushing is documented without separate collection billing
Modifier 52 or 53 supported by explicit limitation/stop reason
Modifier 59 or X{EPSU} used only with a documented distinctness scenario consistent with CMS guidance
PFS pricing and indicators verified through the CMS PFS Look-Up Tool for the service year
Conclusion
CPT 49320 represents diagnostic laparoscopic evaluation, yet payer systems treat it as a high-scrutiny code due to its “separate procedure” status. Clean reimbursement depends on documented diagnostic intent, a detailed survey narrative, and modifier use that matches CMS NCCI criteria. CMS policy places responsibility on the provider record to justify any NCCI-associated modifier appended to bypass an edit.
A workflow that couples a structured op note with a pre-submission checklist turns CPT 49320 into a predictable claim rather than a denial pattern.
FAQ on CPT 49320
What does CPT 49320 report?
CPT 49320 reports diagnostic laparoscopy of the abdomen, peritoneum, and omentum, with or without specimen collection by brushing or washing, and it is labeled as a separate procedure.
Does CPT 49320 require a modifier?
Modifier use depends on context. Standalone diagnostic laparoscopy often needs no modifier. Distinctness scenarios require an appropriate NCCI-associated modifier supported by documentation.
Can CPT 49320 be billed with another laparoscopic procedure?
Separate reporting faces bundling risk due to the “separate procedure” label. Separate reporting requires a distinct scenario supported by documentation and allowed by the payer’s edit logic.
Are brushings and washings billed separately?
Collection by brushing or washing is included in the CPT 49320 descriptor. Separate billing for collection commonly creates denials.
Does Medicare reimburse CPT 49320?
Medicare reimburses covered services per the Physician Fee Schedule. Payment details vary by year, locality, and place of service, and CMS provides the PFS Look-Up Tool for pricing and RVU indicators.
Remote Patient Monitoring (RPM) has delivered real clinical value for years. Billing rules lagged behind real patient behavior. A large gap came from a single threshold that decided everything.
The CY 2026 Physician Fee Schedule (PFS) final rule shifted RPM toward a tiered structure. The rule supports reimbursement tied to clinically meaningful monitoring, not perfect daily adherence.
CPT 99445 is the core fix for the device-supply gap. The code recognizes 2–15 days of physiologic data transmission in 30 days as a billable device supply.
This guide is written for physicians, billing teams, revenue cycle leaders, and RPM program managers who need clean rules, claim-safe documentation, and audit-ready workflows.
What CPT Code 99445 Means
Multiple perspectives matter here because “RPM billing” mixes clinical intent, device rules, and claim rules.
CPT 99445 reports RPM device supply for months with 2–15 days of transmitted physiologic data in a 30-day monitoring period. The code covers the device supply and the capability for daily recordings or programmed alerts to transmit, based on the code descriptor structure used across RPM device-supply codes.
CPT 99445 does not represent provider time. Time-based work uses separate RPM management codes.
CPT 99445 exists because the prior device supply code, 99454, required a minimum number of days that often excluded real-world monitoring patterns. The 2026 update split device supply into two buckets:
99445 for 2–15 days
99454 for 16–30 days
That split gives programs a compliant way to bill stable patients, step-down monitoring, and short episodes such as post-discharge observation.
The 2026 RPM Update at a Glance
Multiple perspectives matter because RPM changes in 2026 touched device supply and management time.
New RPM codes effective January 1, 2026
Two codes matter in daily operations:
CPT 99445: RPM device supply for 2–15 days of data transmission in a 30-day period
CPT 99470: RPM treatment management for 10–19 minutes in a calendar month, with at least 1 real-time interactive communication with the patient or caregiver
Existing RPM codes that still apply
The foundational RPM structure remains active:
99453: device setup and patient education
99454: device supply for 16–30 days
99457: treatment management, first 20 minutes
99458: each additional 20 minutes
The new codes extend the structure. The new codes do not replace the older ones.
Why the Old 16-day Rule Created a Revenue Gap
Multiple perspectives matter because the 16-day rule created both financial and clinical distortions.
The device-supply cliff
Under the older approach, a patient with 15 transmission days produced the same device-supply reimbursement as a patient with 0 days.
Operational reality looked different:
Care teams reviewed transmitted readings on many of those “short” months
Nurses and medical assistants escalated abnormal values.
Physicians changed medications, diet plans, and follow-up intervals.
The work existed. The device remained deployed. Reimbursement failed at a single threshold.
The management-time cliff
Time-based RPM had a similar cliff. Under the older model, 19 minutes of management time failed the 20-minute minimum, leaving brief but meaningful interventions unpaid.
CPT 99470 addresses that time gap by paying a defined bucket for 10–19 minutes when the interactive communication requirement is met.
How CPT 99445 Closes the 2–15 Day Device-Supply Gap
Multiple perspectives matter because short monitoring episodes often match clinical goals better than daily long-duration tracking.
CPT 99445 recognizes a simple truth: clinical relevance does not equal daily frequency.
Short monitoring periods fit common care pathways:
post-discharge stabilization for blood pressure, weight, and pulse oximetry
medication titration periods for antihypertensives and diuretics
stable chronic disease management using periodic checks
adherence-challenged patients who still transmit meaningful data
The key operational change is predictable: months with 2–15 transmission days no longer drop to zero for device supply.
CPT 99445 vs CPT 99454: Correct Code Selection
Multiple perspectives matter because many denials come from simple bucket errors.
The rule that decides everything
The deciding factor is only the number of days with valid transmitted data in the 30-day period.
2–15 days → bill 99445
16–30 days → bill 99454
Diagnosis does not change that bucket rule. The vendor does not change that bucket rule. Provider effort does not change that bucket rule.
Simple billing decision logic
0–1 days of transmitted data → no RPM device-supply code
2–15 days → 99445
16–30 days → 99454
One 30-day period → only one device-supply code
Mutual exclusivity is strict. Billing both device-supply codes in the same 30-day period is a clean audit trigger.
Billing Rules and Requirements for CPT 99445
Multiple perspectives matter because compliance rests on device standards, data standards, and claim standards.
Billing frequency
Bill once per 30 days per patient
Do not bill 99445 and 99454 for the same patient in the same 30-day period.
Qualifying devices
Device qualification is not optional.
CPT 99445 requires an RPM device that meets medical device expectations and supports automatic recording and transmission.
Non-qualifying data sources include:
manual patient entry into an app
text messages with photos of readings
consumer wellness devices without an appropriate medical device status
Common qualifying device categories include blood pressure cuffs, glucometers, weight scales, and pulse oximeters that transmit readings electronically.
Eligible billing practitioners and clinical staff
Physicians and other qualified health care professionals bill the service. Clinical staff perform many RPM tasks under the supervision of rules that apply to RPM services.
Local compliance policies should define supervision level, task delegation, and documentation standards.
Medicare Payment Expectations for CPT 99445 in 2026
Multiple perspectives matter because finance teams need realistic forecasting, not a single national number.
Many RPM summaries report roughly the same national average payment for 99445 and 99454, with an estimated non-facility national average around the mid-$40 range. Locality adjustments apply.
A safe way to state this internally:
Budget at the national average for planning
Load your MAC fee schedule rates in the billing system for real forecasting.
Track non-facility vs facility impacts where applicable
Why CMS valued the buckets similarly
CMS discussed using OPPS cost data to inform rate-setting for some remote monitoring services. Several policy summaries tie that valuation approach to remote monitoring practice expense logic and emphasize auditable data sources.
How CPT 99445 Works with other RPM codes
Multiple perspectives matter because device supply, setup, and management time are separate claim “lanes.”
99445 with 99453 (setup month)
The first month of monitoring often includes setup and education.
Bill 99453 for setup and patient education
Bill 99445 in the same 30-day period when data transmission reaches 2–15 days
Documentation must show the setup activity and the patient education content.
99445 with management-time codes
CPT 99445 covers device supply only.
Management time uses:
99470 for 10–19 minutes with at least one real-time interactive communication
99457 for 20+ minutes with interactive communication requirement
99458 for each additional 20 minutes beyond the first 20
Non-additive rule:
99470 and 99457 are not billed together for the same month.
Real-world Use Cases of CPT 99445
Multiple perspectives matter because use cases drive documentation quality.
1) Post-discharge monitoring
Discharge transitions often involve a short stabilization period.
A common pattern:
14 days of daily blood pressure and weight Week3 and week 4 without readings due to the step-down plan
A 14-day month bills 99445, not 99454.
2) Medication titration
Medication changes need tight observation for a defined window.
Examples include:
antihypertensive dose changes
diuretic adjustments in fluid management plans
A 10-day monitoring window still supports clinical decisions, and the device supply becomes billable in that month through 99445.
3) Stable hypertension monitoring
Stable patients often follow periodic monitoring.
A plan with 3 readings per week yields 12–13 transmission days in many months. That month’s bills are 99445.
4) Weight management programs
Weekly or biweekly weigh-ins reduce burnout and support adherence in obesity programs.
A month with 8 weigh-in bills of 99445.
5) Patients with adherence barriers
Patients who reach 8–12 transmission days remain clinically engaged. 99445 prevents device-supply revenue loss tied to imperfect adherence.
When CPT 99445 is Not Applicable
Multiple perspectives matter because denial avoidance starts with exclusion rules.
CPT 99445 is not billable in these situations:
fewer than 2 days of transmitted data in the 30-day period
data sent through manual entry, photos, or messages rather than automatic transmission
Devices that do not meet medical device expectations for RPM
monitoring without documented medical necessity
Medical necessity documentation should tie monitoring to problems such as hypertension, heart failure, diabetes, COPD, obesity, or post-discharge risk, using diagnoses, symptoms, and treatment-plan goals.
Common denials and audit triggers for CPT 99445
Multiple perspectives matter because audit failure often comes from process gaps, not intent.
Denial trigger 1: missing day count
Claims fail when the record lacks:
start date and end date for the 30-day period
total number of transmission days
source of the count, such as RPM platform logs
Denial trigger 2: non-qualifying data pathway
Manual uploads often look like transmissions inside an EHR note. Auditors treat those as non-qualifying pathways.
Denial trigger 3: code conflicts
High-risk patterns include:
billing 99445 and 99454 in the same 30-day period
billing 99470 and 99457 in the same month
overlapping time with CCM, PCM, or other time-based services
Audit-ready documentation checklist for CPT 99445
Multiple perspectives matter because documentation must satisfy clinical review and claims review.
A clean 99445 record includes 7 items:
30-day monitoring period start date and end date
Transmission-day count for that period.
Physiologic parameters monitored, such as blood pressure, weight, glucose, and oxygen saturation
Device identification, including model name and device status, in your vendor file
Data pathway proof, showing automatic transmission from device to platform
Medical necessity statement, tied to a condition and a monitoring goal
Clinical actions, such as medication changes, patient outreach attempts, threshold alerts, and care plan updates
Documentation quality improves when the RPM platform and EHR share a standard monthly summary note template.
CPT 99445 vs CCM, PCM, and RTM
Multiple perspectives matter because “double counting” creates recoupment risk.
RPM with CCM or PCM
RPM device supply can be billed alongside CCM or PCM. Time-based minutes must remain separated. One minute of staff time counts once.
A strict internal rule:
RPM time log stays inside the RPM module
The CCM time log stays inside the CCM module.
Supervisors review overlap before claims release
RPM vs RTM
RTM tracks therapy adherence and therapy response. RPM tracks physiologic parameters. Code choice depends on the parameter and the device pathway.
RTM policies and codes have their own day buckets and time buckets, separate from RPM.
Medicare vs Commercial payer adoption
Multiple perspectives matter because Medicare policy sets a baseline,, and commercial payers vary.
Medicare established the new RPM code structure for 2026 through the PFS final rule framework. Commercial payers often follow with payer-specific timelines, coverage policies, prior authorization rules, and edits.
A practical control is a payer policy matrix that tracks:
99445 coverage status
prior authorization requirements
frequency limits
modifier rules
denial codes and appeal language
Some payer medical policies already list 99445 within remote physiologic monitoring code sets.
Putting CPT 99445 into your RPM program
Multiple perspectives matter because success needs workflow changes, not just new codes.
System updates
Billing success improves when the system performs 3 actions:
counts transmission days automatically
locks the device-supply code based on the bucket
flags conflicts between 99445 and 99454
Team training
Training should cover:
day thresholds for 99445 vs 99454
time thresholds for 99470 vs 99457 vs 99458
“automatic transmission” definition
medical necessity documentation expectations
Monthly QA and internal audits
A basic QA process catches most errors:
sample 10 charts per month per site
Validate transmission-day count against platform logs. Verify device qualification documentation.
Verify code exclusivity edits.
Verify time separation rules across RPM and CCM.
Conclusion:
CPT 99445 changes RPM economics in a direct way. Months with 2–15 transmission days now support compliant device-supply reimbursement.
Preparation steps that reduce denials:
Implement automated day counting
enforce mutual exclusivity edits
standardize monthly documentation templates
Audit time overlap across RPM and CCM
train staff on 99445 and 99470 thresholds
RPM programs that encode these controls scale faster and face fewer recoupment events.
Frequently Asked Questions
What is CPT 99445 used for?
CPT 99445 reports RPM device supply for months with 2–15 days of transmitted physiologic data in a 30-day period.
How many days are required to bill 99445?
At least 2 days and no more than 15 days in the 30-day period.
Can CPT 99445 and 99454 be billed together?
No. The codes are mutually exclusive for the same 30-day period.
Does CPT 99445 require interactive communication?
No. Interactive communication applies to RPM management codes such as 99470 and 99457.
How much does Medicare pay for CPT 99445 in 2026?
Many summaries cite a national average estimate in the mid-$40 range, with locality variation, and a similar valuation to 99454.
Can CPT 99445 be billed with CCM codes?
Yes. Time minutes must not be counted twice across RPM and CCM.
Respiratory billing accuracy improves when clinical workflow, coding rules, and payer edits are treated as one system. CPT 94010 sits at the center of outpatient spirometry revenue, yet denials keep appearing for the reasons of missing interpretation, thin medical necessity, and documentation gaps that fail payer review standards.
This guide focuses on denial prevention, audit exposure, and payer behavior. The goal is to clean claims the first time, with documentation that stands up to post-payment review.
What CPT Code 94010 Means
Billing clarity improves when the CPT descriptor is translated into what payers expect to see in the chart. CPT 94010 describes spirometry with a graphic record and measurement of vital capacity and expiratory flow rates, with or without maximal voluntary ventilation. Respiratory coding guidance notes that pulmonary diagnostic testing codes in the 94010–94799 range include the laboratory procedure and the interpretation of test results.
CPT Code 94010 Description
Claim implication: A paid 94010 claim assumes two pieces exist in the record:
Professional interpretation: physician review with a written report and signature
Medicare contractor billing-and-coding guidance is explicit: “All studies require an interpretation with a written report,” and computerized reports require a physician signature attesting to review and accuracy.
What 94010 Includes and Excludes
Coding precision improves when “included” and “not included” are treated as denial triggers rather than academic definitions.
Services included in 94010
Documentation and coding align under 94010 when the encounter contains:
Spirometry without bronchodilator responsiveness testing
Graphic record retained in the record (flow-volume loop)
Physician interpretation and written report with signature
Services excluded from 94010
Revenue protection improves when unbundling patterns are eliminated:
Pre- and post-bronchodilator testing (belongs under 94060, not 94010)
Separate reporting for bronchodilator administration that is already included in 94060
Separate reporting for items payer edits treat as bundled into spirometry in the same encounter (payer and NCCI dependent)
Respiratory coding guidance lists code-pair exclusions such as “Do not report 94010 with 94150, 94200, 94375, 94728.”
Clinical Use Cases That Support Medical Necessity
Medical necessity is a charting problem before it becomes a coding problem. Medicare contractor guidance states that ICD-10 codes must reflect the patient’s actual condition, and a diagnosis listing alone does not justify the test without a supportive context.
Clinical documentation supports spirometry billing when it ties testing to an active decision point, such as:
Disease assessment (examples: asthma control assessment, COPD baseline characterization, interstitial lung disease monitoring during a management change)
Preoperative respiratory risk assessment with stated indication
Chart language that pays better than symptom-only charting
“Dyspnea on exertion with reduced exercise tolerance; spirometry ordered to quantify airflow limitation and guide therapy selection.”
“COPD follow-up with change in symptoms; spirometry ordered to reassess obstruction severity and adjust inhaler regimen.”
Medicare contractor guidance supports follow-up testing only under clinically required circumstances, giving an example that weekly or monthly PFT follow-up fits periods such as acute exacerbation of interstitial lung disease.
When 94010 Should Not Be Reported
Audit resistance improves when overuse patterns are stopped at scheduling rather than appealed after denial.
Avoid reporting 94010 for:
Screening or routine testing without a documented medical necessity context
Same-day repeat testing without documented justification and correct repeat-service modifier usage
Encounters that include bronchodilator responsiveness testing (use 94060)
CPT 94010 vs 94060 and Related PFT Codes
Denial rates drop when coders treat pulmonary codes as mutually exclusive building blocks.
94010 vs 94060 (bronchodilator responsiveness)
CPT 94060 describes bronchodilation responsiveness testing and explicitly references spirometry “as in 94010” with pre- and post-bronchodilator administration. NCCI policy states that 94060 includes bronchodilator administration and flags misuse of separate inhalation treatment coding to bill administration that is already included.
Claim behavior to expect
Billing 94010 + 94060 in the same session tends to hit bundling edits because baseline spirometry is integral to the bronchodilator study logic.
Billing separate bronchodilator treatment administration with 94060 creates compliance exposure under NCCI guidance.
Other codes frequently confused with 94010
Respiratory coding guidance highlights code-pair conflicts and bundling exclusions around spirometry and related testing (examples: flow-volume loop codes, MVV codes, lung volume codes). Coding should match the performed study type and the retained outputs in the record.
ICD-10 Selection That Payers Accept
Claims integrity improves when ICD-10 selection answers one question: Why was spirometry needed on this date? Medicare contractor guidance states the clinical context must support the necessity beyond the code label.
Common diagnosis groupings used to support spirometry include:
Obstructive disease diagnoses (examples: asthma family J45.x, COPD family J44.x)
Symptom-only claims with no clinical narrative (payer view: “testing not justified”)
Non-specific codes without specificity available in the note
Diagnosis mismatch between order, assessment, and claim
Modifier Guide for CPT 94010
Modifier accuracy improves when each modifier is tied to a distinct payer question.
Modifier 26 (Professional Component)
Use -26 when the provider bills interpretation only and another entity bills the technical component.
Modifier TC (Technical Component)
Use -TC when billing the technical performance only (equipment/tech/time),and interpretation is billed elsewhere.
Respiratory coding guidance reinforces that pulmonary diagnostic testing codes include interpretation, so component billing requires clean separation and documentation of who did what.
Modifier 25 (Separate E/M)
Use -25 on the E/M code when a significant, separately identifiable evaluation occurred beyond test performance and result review. NCCI policy describes modifier -25 use when E/M work is “above and beyond” procedure work.
Modifier 59 (Distinct Procedural Service)
Use -59 only when payer edits allow separation and documentation proves distinct services at distinct encounters or distinct anatomic/testing contexts. Overuse increases audit probability.
Modifiers 76 and 77 (Repeat Procedure)
Use -76 for same provider repeat testing, -77 for different provider repeat testing, with documented justification tied to a clinical change or a failed/invalid study.
Modifiers 52 and 53 (Reduced/Discontinued)
Use -52 for reduced services and -53 for discontinued procedures, with documentation stating what stopped and why.
Medicare Billing Rules That Drive Denials
Medicare payment stability improves when documentation is built to withstand post-payment review. Medicare contractor guidance for respiratory care billing and coding states:
An order/referral with diagnoses and requested tests should be on file
Spirometry studies require 3 attempts to be clinically acceptable
All studies require interpretation with a written report.
Computerized reports require a phphysician’signature attesting to review
Documentation must show test results and use in treatment.
Denial prevention improves when these points become part of the spirometry workflow, not billing cleanup.
Supervision and Place of Service: Office vs Facility Differences
Compliance improves when supervision rules are treated as a billing prerequisite rather than a staffing detail.
What “supervision” means under federal rules
Federal regulation defines:
General supervision: overall direction and control; physician presence not required during performance
Direct supervision: physician present in the office suite and immediately available
Personal supervision: physician in the room during performance
A CMS transmittal listing diagnostic test supervision levels includes pulmonary codes and shows a supervision indicator for 94010 (technical component) and 94060 (technical component), supporting the operational reality that bronchodilator responsiveness studies are treated with tighter supervision expectations than simple spirometry.
Operational rule that reduces risk
Schedule and staff spirometry with supervision level verified in the Medicare Physician Fee Schedule database for the code and setting, then align clinic policy, staffing, and signatures to that requirement.
Commercial Payer Considerations
Contract compliance improves when commercial payer policies are treated as separate rulebooks. Payers publish utilization limits, documentation requirements, and recoupment language in medical and payment policies. A national payer policy for pulmonary function testing warns that missing requirements can trigger denials and recovery of incorrectly paid claims.
Commercial payer realities
Frequency edits can be stricter than Medicar..e
Prior authorization is uncommon for basic spirometry, but medical policy documentation requirements still apply.
Post-payment audits remain active even after the initial payment.
Documentation Checklist for Efficient 94010 Billing
Audit safety improves when every spirometry encounter generates the same minimum documentation package.
Chart elements to include every time
Order/referral or documented intent tied to assessment/plan
Denial reduction improves when root causes are converted into front-end controls.
Denial driver: Missing interpretation
Control: Lock claim submission until a signed interpretation is present
Denial driver: Weak medical necessity
Control: Require an indication statement tied to assessment and plan, not a symptom label alone
Denial driver: Bundling conflicts (94010 vs 94060, add-on inhalation treatment)
Control: Build charge rules aligned to NCCI policy on 94060 and bronchodilator administration inclusion
Denial driver: Utilization outliers
Control: Track repeat spirometry intervals; Medicare contractor guidance limits frequent follow-up to clinically required periods
Industry denial pressure is rising across practices, with MGMA polling showing many medical group leaders reporting increased denial rates compared to the prior year.
NCCI Bundling Explained
Clean coding improves when “most comprehensive code” is treated as the default. NCCI policy instructs reporting the most comprehensive code and avoiding unbundling.
Practical application
Bronchodilator responsiveness testing belongs under 94060, which describes spirometry as in 94010 plus pre/post bronchodilator administration..
Separate reporting for bronchodilator administration that is already included in 94060 creates exposure under NCCI guidelines. c.e
Patient Explanation That Supports Coverage
Coverage improves when patients understand denials often reflect documentation, not clinical need. Medicare contractor guidance requires the record to document results and usage in treatment, which mirrors what payers expect in appeals.
Patient-facing summary
Spirometry measures airflow and lung volumes through forced breathing maneuvers.
The chart must contain results, physician interpretation, and the clinical reason the test was ordered.
Insurance denials frequently point to missing signatures, missing interpretation, or unclear diagnosis linkage rather than a dispute over the test itself.
Conclusion
Denial prevention improves when documentation, coding, and supervision rules are engineered intthe o workflow. Medicare contractor guidance requires orders/referrals, acceptable spirometry attempts, and signed interpretations, and NCCI policy clarifies bundling logic around bronchodilator responsiveness testing.
Revenue protection follows from a repeatable process:
Document necessity tied to a decision point
Capture graphic output and quantitative values.
Finalize a signed interpretation before claim release.
Code the most comprehensive service performed.
Monitor utilization intervals and modifier usage for outliers.
FAQs
What is included in CPT 94010?
CPT 94010 describes spirometry with a graphic record and airflow/volume measurements. Medicare contractor guidance requires interpretation with a written report and physician signature, and spirometry studies require 3 attempts to be clinically acceptable.
How many times can CPT 94010 be billed in one day?
Same-day repeats require documentation that supports the necessity and repeat-procedure modifier use where appropriate. Medicare contractor guidance flags frequent follow-up testing as appropriate only when clinically required.
Can CPT 94010 and 94060 be billed together?
NCCI policy describes 94060 as bronchodilation responsiveness testing with spirometry, “as in 9401,” which drives payer bundling behavior and makes same-session reporting of both codes high risk.
Which modifiers apply to CPT 94010?
Component modifiers (-26, -TC) apply when interpretation and performance are split across entities. Modifier -25 applies to a separately identifiable E/M beyond procedure work, consistent with NCCI principles. Repeat-service modifiers (-76, -77) apply for repeat testing with documentation.
Why do 94010 claims get denied?
Medicare contractor guidance highlights missing supportive documentation as a denial driver, including a lack of documented necessity context, missing interpretation/signature, and inadequate spirometry attempt documentation. Payer medical policies warn about denials and recovery when requirements are not met.
Does Medicare cover spirometry?
Medicare contractor guidance supports coverage when documentation supports medical necessity, orders/referrals are present, and interpretation/reporting requirements are met.
What supervision level applies to 94010?
Federal regulation defines general/direct/personal supervision for diagnostic tests. A CMS transmittal lists supervision indicators for pulmonary diagnostic tests, including 94010 (technical component) and 94060 (technical component). Site-specific verification in the Medicare fee schedule database remains a standard compliance step.
Neurology claims fail for 2 reasons: the clinical record does not match the CPT descriptor, or the claim line does not follow the code’s billing rules. CPT 95886 sits in the middle of that problem. The study may be performed correctly, and the report may read well, yet payment still drops because the claim does not prove the “complete” extremity electromyography (EMG) criteria, or the payer does not see the required primary nerve conduction study (NCS) on the same date of service. AANEM guidance and coding education documents describe the same pattern: denials follow missing completeness elements, missing NCS linkage, and unit errors.
CPT 95886 Simplified: What the Service Represents
CPT 95886 represents a needle electromyography (EMG) study of one extremity (one arm or one leg), with related paraspinal muscles included when performed, done in the same session as a separately reportable nerve conduction study. Coding references describe it as a complete extremity needle EMG.
Needle EMG records electrical activity from selected muscles using a fine needle electrode. The interpreting clinician evaluates findings such as insertional activity, spontaneous activity, motor unit action potentials, and recruitment patterns. Those elements support diagnostic conclusions for conditions such as radiculopathies, mononeuropathies, plexopathies, motor neuron diseases, and myopathies. EMG documentation guidance in coverage and policy materials emphasizes that muscle selection and interpretation occur during the examination, not after it.
The Add-On Rule: Why CPT 95886 Cannot Stand Alone
Coding compliance for 95886 starts with its status as an add-on code. Add-on reporting means 95886 is not the “main” procedure line. The claim must include a qualifying primary NCS code on the same date of service. Coding guidance and electrodiagnostic billing education sources describe 95886 as “list separately in addition to code for primary procedure,” and they pair it with the NCS code family 95907–95913.
AANEM policy language states the same operational rule: report 95886 only when EMG testing and NCS are performed on the same day.
Practical claim impact
A claim line for 95886 without an NCS line often triggers:
denial for “incorrect coding,”
denial for “invalid code combination,” or
downcoding to a limited service based on payer policy.
The cleanest prevention method is simple: treat 95886 as a dependent line item and verify the NCS line is present, dated the same day, and linked to the same clinical indication.
Complete EMG Criteria: The Measurable Threshold Payers Expect
Payers do not accept “complete” as a narrative label. Completeness is measured.
AANEM recommended policy describes CPT 95886 completeness using these criteria:
Minimum of 5 muscles studied per limb, and
Muscles must be innervated by 3 distinct nerves (examples listed in AANEM guidance include radial, ulnar, median, tibial, peroneal/fibular, femoral) or represent 4 spinal levels.
Educational coding references use the same threshold language.
What does “5 muscles” mean in documentation?
A payer reviewer needs to see a muscle list that makes the threshold obvious. A complete extremity note typically shows:
muscle names (not “proximal” or “distal” only),
laterality (right/left),
extremity location (upper/lower),
Findings for each muscle are tested.
Muscle repetition does not replace breadth. Testing 5 sites that map to the same pathway does not read as 5 diagnostically distinct muscles for coding purposes. AANEM policy highlights nerve-level representation, not sub-branches, as part of correct completeness reporting.
CPT 95886 vs CPT 95885: Denial Reasons
CPT 95885 represents a limited extremity needle EMG. CPT 95886 represents a complete extremity needle EMG with the 5-muscle threshold and nerve/spinal-level breadth. Coding change summaries and electrodiagnostic billing guides define this difference in the descriptor-level language.
A billing-safe decision rule
Report 95885 when the extremity EMG includes 4 or fewer muscles.
Report 95886 when the extremity EMG includes 5 or more muscles and meets the 3-nerve or 4-spinal-level representation.
Downcoding risk rises when the report reads “complete study” but lists 3–4 muscles, or lists 5 muscles without showing nerve/spinal-level distribution.
Per-Extremity Reporting and Unit Logic
CPT 95886 is reported per extremity. One unit represents the complete needle EMG work for one limb, with or without related paraspinal muscles, as performed and documented. AANEM policy states that “one unit includes all muscles tested in a particular extremity.”
Multi-limb encounters
A four-limb study can produce multiple EMG units across extremities, and AANEM policy notes a combined maximum of four units across 95885 and 95886 when all extremities are tested.
Claim integrity depends on matching units to:
the number of limbs tested,
the muscle list per limb,
The medical necessity narrative per limb (symptoms and exam findings often differ by extremity).
A payer reviewing the chart expects each billed extremity to have its own muscle set and clinical reason.
Documentation Practices: A Denial-Resistant Checklist
A reviewer reads the record in two passes: “Was the service reasonable?” and “Does the documentation match the code?” Documentation elements from payer and policy materials align on the same core pieces.
Use this checklist to align the report with CPT 95886:
1) Clinical indication stated in concrete terms
Document symptoms and functional impact using specific plural nouns, such as:
numbness, tingling, burning pain,
weakness, foot drop, grip loss,
gait instability, hand clumsiness.
2) Exam or referral context
List objective findings that drove testing, such as:
sensory loss distribution,
reflex asymmetry,
strength deficits by myotome.
3) NCS performed the same day
List the NCS component and interpretive summary in the same final report packet, because 95886 is reported in addition to the primary NCS procedure.
4) Muscle list that proves completeness
Include:
at least 5 muscles for that extremity,
laterality,
distribution across 3 nerves or 4 spinal levels.
5) Needle EMG findings per muscle
Document the standard interpretive elements:
insertional activity,
fibrillation potentials or positive sharp waves,
motor unit morphology,
recruitment pattern.
6) Physician interpretation and impression
State the diagnostic conclusion in clear terms, such as:
cervical radiculopathy level,
lumbosacral plexopathy pattern,
length-dependent polyneuropathy features.
7) Signature and date of service alignment
A mismatch between the performance date, interpretation date, and billed date can trigger technical denials even when the content is strong.
Clinical Scenarios That Commonly Fit CPT 95886
Coverage and professional policy documents frame needle EMG as part of a diagnostic pathway for nerve and muscle disorders, not a screening tool.
Common billed scenarios that align with a complete extremity study include:
Cervical radiculopathy evaluation
Symptoms often include neck pain radiating into the arm, numbness in a dermatomal pattern, and weakness in shoulder abduction, elbow extension, or wrist extension. A complete extremity EMG documents multiple limb muscles and may include paraspinals related to the suspected root level.
Diabetic polyneuropathy staging
Symptoms often include distal numbness, burning pain, nocturnal cramps, and balance problems. A complete extremity needle exam supports severity characterization when paired with NCS results and documented distal-to-proximal spread.
Sciatic or peroneal neuropathy workup
Symptoms often include foot drop, tripping, toe drag, and dorsum-foot sensory loss. A complete extremity study documents a muscle set that separates radiculopathy, plexopathy, and focal mononeuropathy patterns.
Clinical validity still depends on documentation. A complete code without complete documentation reads as overcoding during audit.
ICD-10 Diagnosis Selection: Link the Code to the Scope of Testing
Diagnosis coding must match the reason a complete study was required. A complete extremity EMG implies complexity or diagnostic uncertainty that needs broad sampling.
Examples of ICD-10-CM codes that commonly appear with electrodiagnostic testing include:
G56.0- (carpal tunnel syndrome variants by laterality),
G57.0- (sciatic nerve lesion variants),
G54.1 (lumbosacral plexus disorders),
G62.9 (polyneuropathy, unspecified),
E11.42 (type 2 diabetes mellitus with diabetic polyneuropathy),
G12.21 (amyotrophic lateral sclerosis).
Diagnosis linkage errors that trigger denials include:
using a focal entrapment diagnosis for a four-limb complete workup without additional indications,
omitting symptom codes when the definitive diagnosis is not established at the time of testing,
linking all limbs to one diagnosis without documenting bilateral symptoms.
Repeat Testing and Frequency Controls:
Repeat EMG/NCS is reviewed through a medical necessity lens. Payer policies describe repeat testing as appropriate under defined clinical changes, not as routine follow-up. Priority Health lists rationales such as new symptoms, unclear results, fast-changing diseases, monitoring disease course, and recovery tracking, with documentation expected for the rationale.
Some payer policies describe time-based expectations, often stating repeat testing within a 12-month period is not expected in most cases unless documented exceptions apply.
A repeat-testing note should state:
What changed since the last study (symptoms, exam findings, treatment response)?
What decision does the repeat study support (surgical planning, medication shift, prognosis)?
Routine repetition without that narrative often denies, even when the study itself is complete.
Major CPT 95886 Billing Mistakes and their Solution
Mistake 1: Billing 95886 without an NCS primary code
Solution: Add the qualifying NCS line on the same date of service and keep it linked to the same indication. AANEM policy and billing education sources describe same-day pairing as required for reporting 95886.
Mistake 2: Calling a 4-muscle study “complete.”
Solution: Report 95885 for 4 or fewer muscles, and reserve 95886 for 5 or more muscles with the required nerve/spinal breadth.
Mistake 3: Missing muscle list detail
Solution: List each muscle with laterality and findings. Avoid grouped phrases like “upper extremity muscles tested.”
Mistake 4: Wrong unit reporting across extremities
Solution: Match units to limbs tested and document each extremity separately. AANEM policy clarifies that one unit includes all muscles tested in one extremity, and combined reporting across extremities is commonly capped at four units across 95885/95886.
Mistake 5: Diagnosis-code mismatch with the scope of testing
Fix: Align the diagnosis with the clinical question that required broad sampling, and document symptom distribution by limb.
Reimbursement Policies
Payment varies by payer, site of service, and components of the billing structure.
Medicare payments under the Physician Fee Schedule are built from work, practice expense, and malpractice RVUs, multiplied by a conversion factor, with geographic adjustments applied. CMS explains this RVU-to-payment framework in its Physician Fee Schedule materials and CY 2026 final rule fact sheet.
Site of service changes payment because practice expense differs between facility and non-facility settings. Contracted commercial rates differ from Medicare, and prior authorization rules can add a separate gate even when documentation is strong.
A billing workflow that reduces surprises uses two checks:
Verify payer policy for electrodiagnostic studies before scheduling repeat testing.
Verify current-year fee schedule inputs (RVUs and conversion factor) during annual updates.
Conclusion: Code Definition Discipline Prevents Most 95886 Denials
CPT 95886 pays cleanly when the record proves three facts: an NCS primary procedure occurred the same day, the limb study met the complete threshold, and the documentation shows muscle selection plus interpretive findings. Professional policy documents and billing education references converge on the same measurable rules: add-on reporting, 5+ muscles, and 3 nerves or 4 spinal levels per extremity.
FAQs
Is CPT 95886 a complete EMG study?
CPT 95886 is defined and taught as a complete extremity needle EMG with a minimum of 5 muscles, meeting nerve or spinal-level distribution criteria.
Can CPT 95886 be billed without nerve conduction studies?
Reporting guidance describes 95886 as an add-on code reported in addition to a primary NCS procedure performed the same day.
What is the difference between CPT 95885 and CPT 95886?
CPT 95885 is limited (4 or fewer muscles). CPT 95886 is complete (5 or more muscles with required nerve/spinal breadth).
How do payers verify that CPT 95886 meets the “complete EMG” requirement?
Payers review the muscle list, laterality, and nerve or spinal-level distribution documented in the report. A valid CPT 95886 claim must clearly show at least five distinct muscles per extremity and representation across three nerves or four spinal levels, along with interpretive findings for each muscle. Missing these elements leads to downcoding or denial.
What triggers a denial even when CPT 95886 documentation looks clinically correct?
Denials often occur when billing rules are not followed despite proper clinical performance. Common triggers include absence of a same-day nerve conduction study (NCS), incorrect unit reporting per extremity, or diagnosis codes that do not justify a complete study. Claim structure and code linkage must align with documentation to secure reimbursement.
CPT code 92014 looks simple in a code list. Real-world payment rules make it the easiest for the ophthalmology and optometry codes. Billing risk grows because payers do not judge 92014 by “number of tests performed.” Payers judge 92014 by medical necessity, documentation language, diagnosis linkage, utilization pattern, and editing rules.
Practices meet the clinical intent of a comprehensive exam but still fail payer expectations because the chart does not show initiation or continuation of a diagnostic and treatment program, which is the core concept behind the eye codes.
This blog covers each section using 3 perspectives: CPT definition, Medicare coverage structure, and commercial payer editing behavior.
CPT 92014 Description
92014 reports a comprehensive ophthalmological service for an established patient that includes a medical examination and evaluation with initiation or continuation of a diagnostic and treatment program.
What “Comprehensive Ophthalmological Service (Established Patient)” means
1. Comprehensive Ophthalmological Service
A complete eye evaluation that examines multiple aspects of the visual system—not a limited or problem-focused exam.
It includes:
General medical observation
External and ophthalmoscopic examination
Gross visual fields and basic sensorimotor evaluation
Often includes dilation, slit lamp exam, and IOP measurement
The exact elements are not strictly checklist-based like E/M codes but must support a full evaluation of the eye system.
2. Established Patient
A patient who has received professional services from the same physician (or same specialty/group) within the last 3 years.
3. Medical Examination and Evaluation
A clinically necessary assessment, not just a routine vision check. Includes:
Patient history
Clinical findings
Medical decision-making
4. Initiation or Continuation of Treatment
There must be active management, such as:
Starting treatment (e.g., medication for glaucoma)
Adjusting existing therapy
Ordering/interpreting diagnostic tests
5. One or more visits
The comprehensive service may occur in a single visit or across multiple encounters if clinically required.
What CPT 92014 means in AMA style
Coding for 92014 depends on 3 realities: the eye code definition, the “established patient” status rule, and the difference between examination content and clinical management.
1) “Established patient” is a time-and-specialty rule
CPT’s established patient concept uses the 3-year (36-month) lookback tied to professional services by the same physician or another clinician of the same specialty/subspecialty in the same group.
Billing risk shows up when the scheduling system labels a patient “return” while the coding rule labels the patient “new.” Practice management systems often track “new to the practice,” not “new to the specialty/subspecialty under CPT rules.”
Operational fix
Build a registration prompt that checks: same specialty + same group + professional service + past 36 months.
Route edge cases to a coder before checkout.
2) 92014 is not an E/M code
Eye codes (92002–92014) sit in “general ophthalmological services.” They do not use 2021+ E/M time/MDM selection rules. Medicare contractors publish guidance comparing when to use eye codes versus E/M codes based on visit purpose and documentation approach.
Billing implication
A chart that reads like a general medical follow-up note with minimal eye-specific exam detail often performs better under 99213–99215 than under 92014. A chart that reads like a full ophthalmic exam with a defined eye-care plan aligns better with 92014.
3) “Comprehensive” means clinical scope plus management, not test volume
AAO and Medicare contractor descriptions list typical comprehensive exam components such as history, general observation, external and ophthalmoscopic exams, gross visual fields, and basic sensorimotor evaluation.
Payers deny 92014 when documentation shows equipment-driven testing but does not show clinical synthesis. A list of normals does not equal a comprehensive service unless the record shows why the comprehensive service was required and what decision resulted from it.
The core payer question: Did the visit continue or start a diagnostic and treatment program?
Payment accuracy for 92014 depends on 3 perspectives: the CPT concept, medical necessity rules, and the treatment-plan signal in the note.
The phrase “initiation or continuation of a diagnostic and treatment program” is the line payers look for in substance, not wording. A payer-friendly record shows at least 1 management action tied to the diagnosis assessed.
Management actions that support 92014
Use consistent verbs that show active management:
Prescribed medications such as prostaglandin analogs, topical steroids, and antihistamines
Adjusted therapy, such as dose change, stop/start, taper plan
Ordered diagnostics such as OCT, automated visual fields, and fundus photography when diagnosis-driven
Referred to subspecialty or coordinated care with PCP/endocrinology when medically relevant
Planned procedures such as laser, injections, and surgery with a documented decision pathway
Set follow-up timing tied to risk level, such as 2 weeks, 6 weeks, 3 months, based on findings.
A record that ends with “RTC 1 year” without a risk-based reason often reads as routine care in payer logic.
Medical Necessity of CPT Code 92014
Coverage accuracy for 92014 depends on 3 realities: Medicare statutory exclusions, payer benefit design, and diagnosis selection.
Medicare in Routine Refractive Services
Medicare excludes payment for eye examinations performed for the purpose of prescribing, fitting, or changing eyeglasses or contact lenses for refractive errors. CMS documents describe this exclusion, and Medicare contractor education repeats that the determination of refractive state (CPT 92015) is statutorily excluded.
This matters because many denials happen when the note reads like a refraction-driven visit with a medical code attached.
Documentation Signals that Trigger Payer Concerns
Chief complaint documented as “annual exam” with no disease assessment
Assessment limited to refractive error codes or Z codes without symptom or disease workup.
Plan limited to glasses/contact lens update without medical management.
A medical exam still needs a diagnosis-driven reason on that date
A patient can have glaucoma, diabetes, or AMD in the problem list. That fact alone does not prove medical necessity for a comprehensive exam today. The chart needs a reason, such as;
change in symptoms such as blur, floaters, flashes
change in clinical risk, such as IOP drift, optic nerve change
surveillance interval based on disease staging
medication monitoring such as steroid response, glaucoma drop tolerance
Documentation Requirements
Defensibility for 92014 depends on 3 parts of the note: history, exam, and plan language that links to the diagnosis.
1) History that supports the exam scope
Document history in a way that forces diagnosis linkage:
Chief complaint tied to disease or symptom
HPI showing duration, severity, modifying factors, and relevant negatives
Relevant systemic history, such as diabetes control, autoimmune disease, a nd steroid use
Medication list with ocular meds and adherence issues
A payer reads history as the “why” behind the exam.
2) Exam findings that match the comprehensive intent
A comprehensive service should show a structured exam record. Templates work if the content is patient-specific.
Include:
Visual acuity with correction status
IOP method and values
Pupils, EOMs, and confrontation fields were performed.
Anterior segment findings
Posterior segment findings
Optic nerve and macula findings when relevant to diagnosis
Dilation is not mandatory in every clinical situation. A record needs a documented reason when dilation is not performed, such as narrow angles, allergy, patient refusal, or safety constraints tied to the visit context.
3) Assessment and plan that prove active management
Write the plan in a way that makes the “diagnostic and treatment program” obvious:
Diagnosed: primary condition + status such as stable, progressing, suspected
Interpreted: key findings that changed risk, such as RNFL thinning and IOP trend
Managed: medication decision, test order, referral, procedure plan
Scheduled: follow-up interval tied to disease stage and risk
A payer can disagree with a clinical decision. A payer has less room to deny when the decision exists and is tied to the diagnosis.
ICD-10 Pairing: How Diagnosis Impacts 92014 Selection
Claim success depends on 3 diagnosis behaviors: selecting active problems, avoiding benefit-triggering Z codes, and matching laterality/staging when applicable.
Diagnoses that commonly support medical eye care
Examples include:
glaucoma and glaucoma suspect codes
diabetic retinopathy codes with staging
age-related macular degeneration codes
cataract when evaluated for surgery planning
ocular inflammation and infection codes
visual field defect and symptom codes when workup is active
The diagnosis selection must explain why the exam needed a comprehensive scope. Symptom codes can support medical necessity during evaluation. Z codes alone often read as screening or routine care in payer edits.
Modifiers for 92014 CPT Code
Modifier accuracy depends on 3 risks: laterality, separate services, and global surgery rules.
LT / RT / 50: follow the payer’s format
Laterality requirements vary by payer. Some want RT/LT, some want bilateral, and some want units. A clearinghouse rule does not replace payer rules.
Modifier 25: use only with a truly separate E/M service
Modifier 25 applies to a separate, significant E/M service on the same date as a procedure. Automatic 25 use is a common audit pattern because it spikes utilization metrics.
A defensible same-day claim shows:
separate problem that required E/M work beyond the eye exam service, and
separate documentation that stands alone.
Global surgery edits and NCCI logic still matter
CMS NCCI policy explains that separate reporting of E/M services around procedures is limited by global surgery rules and edit logic.
Even when a claim is technically payable, bundling logic can trigger denials that require appeal. Build edit checks for same-day procedures, post-op periods, and payer-specific policies.
Reimbursement Rates: Why the 92014 Payment Varies
Payment predictability depends on 3 factors: Medicare locality, facility setting, and contract terms.
CMS pays physician services under the Medicare Physician Fee Schedule, and rates vary by locality and other factors. Commercial plans vary more because contract rates, carve-outs, and bundled payment policies differ by employer plan and network.
Underpayment control
Compare paid amounts to contracted allowed amounts each month.
Track CPT 92014 paid rate by payer, plan, and site of service.
Appeal systematic underpayment with contract evidence.
Frequency Limits: Understanding Payer Behavior
Many commercial payers apply frequency edits that behave like “1 per 12 months” for detailed eye exams under certain benefits. Medicare does not treat medically necessary eye care as an annual routine benefit, so frequency denials under Medicare often reflect documentation and coverage framing, not a hard annual limit.
Claim defense strategy
Document why today’s exam differs from a routine annual visit.
Tie follow-up timing to disease staging and risk.
Avoid scheduling language like “annual” in medical disease follow-ups.
Chart gap: exam looks intermediate, or the plan lacks management action.
2) Denied for medical necessity
Chart gap: chief complaint and diagnosis do not justifythe vast scope.
3) Denied as routine vision care
Chart gap: assessment focuses on refractive error; plan focuses on glasses/contact lenses.
4) Denied for frequency
Chart gap: no documentation showing disease progression, new symptoms, or risk change.
5) Denied in the global period
Chart gap: post-op care billed separately without documentation meeting global surgery exceptions.
6-Step Approach to Reduce Denials
Billing consistency depends on 3 systems: front-desk capture, technician documentation discipline, and provider plan language.
Step 1: Intake for medical purposes
Capture the chief complaint as a symptom or disease follow-up.
Capture systemic status such as A1c, steroid use, and anticoagulants when relevant.
Step 2: Technician template that supports, not replaces
Document performed components.
Flag contraindications such as dilation refusal.
Step 3: Provider assessment written as decisions
State disease status.
State what changed or what risk was assessed.
Step 4: Plan written as management actions
Prescribe, adjust, order, refer, and schedule with clinical rationale.
Step 5: Coding cross-check
Confirm established status.
Confirm ICD-10 supports medical necessity.
Confirm modifiers match payer rules.
Step 6: Post-bill analytics
Track denial reason codes.
Track downcode rates.
Track frequency edits by payer.
Telehealth Note: Treat 92014 as in-person unless a payer policy states
Telehealth billing depends on explicit payer permission. During the COVID-19 emergency, industry guidance highlighted telemedicine use for some eye codes, such as 92012/92002, under certain conditions, which signals that payer rules for eye codes in telehealth are narrow and policy-driven. A practice should use a written payer policy and POS/modifier requirements for telehealth, including CMS POS guidance.
Conclusion:
CPT 92014 rewards documentation that shows a completed exam and a continuing or initiated diagnostic/treatment program. Risk increases when templates list exam components but omit diagnosis-driven rationale and management decisions. Risk increases when scheduling language implies routine care. Risk increases when the ICD-10 pairing fails to explain medical necessity.
A practice that aligns chief complaint → exam scope → assessment → plan → diagnosis linkage reduces denials, reduces downcodes, and improves appeal outcomes. Coding 92014 less often is not the goal. Coding 92014 with a chart that pays on the first submission is the goal.
FAQs
What does CPT code 92014 mean?
CPT 92014 reports a comprehensive ophthalmological service for an established patient with medical examination and evaluation tied to initiation or continuation of a diagnostic and treatment program.
What is the difference between 92014 and 92012?
92014 represents a comprehensive service. 92012 represents an intermediate service with a more limited scope. Medicare contractors and ophthalmology guidance discuss choosing eye codes versus other options based on documentation and visit purpose.
Can 92014 be billed without dilation?
A comprehensive exam does not require dilation in every clinical situation. Documentation should state why dilation was not performed and how the exam remained medically appropriate for the visit’s purpose.
What is the CPT code for a full eye exam?
92014 applies to an established patient’s comprehensive ophthalmological service. 92004 applies to a new patient’s comprehensive ophthalmological service.
How often can CPT 92014 be billed?
Frequency depends on payer edits and medical necessity. Commercial plans may apply frequency limits under certain benefits. Medical necessity documentation supports additional visits when disease risk and management require them.
Why is eye refraction not covered by insurance?
Traditional Medicare excludes determination of refractive state and routine refractive services from Part B coverage, which is why refraction is commonly patient-pay.
Are you facing revenue loss due to an incorrect CPT 90686 coding issue? I solved this problem. I’ve worked with clinics that administered hundreds of flu shots in a season, only to realize months later that claims were denied, underpaid, or never processed because of small mistakes, missing administration codes, wrong modifiers, or incomplete documentation. Most of the time, the vaccine was given correctly, but the billing wasn’t. That gap between clinical care and correct coding is where practices lose money without even noticing.
Over the years, I’ve seen medical coders, billers, and even experienced practice managers struggle with the same questions: when exactly to use CPT 90686, how it differs from other flu vaccine codes, and why payers reject claims that they “look right.” This guide is based on that real-world experience. The goal is not just to define the code but to help you understand it in a way that prevents denials, protects revenue, and makes flu-season billing predictable instead of stressful.
What is CPT Code 90686
CPT Code 90686 is one of the most common sources of silent revenue loss during flu season. Many providers administer hundreds of influenza vaccines each year, only to discover months later that claims were denied, underpaid, or never processed. In most cases, the vaccine was administered correctly, but the billing was not.
I’ve worked directly with clinics, pediatric practices, OB/GYN offices, and community health centers facing this exact issue. Small mistakes such as missing administration codes, incorrect modifiers, or incomplete documentation can quietly drain revenue. This guide is based on real billing experience and is designed to help you prevent denials, protect reimbursement, and make flu-season billing predictable.
Official Description of CPT Code 90686?
CPT Code 90686 is identified under the Vaccines and Toxoids section and is applied by the American Medical Association (AMA). It is a quadrivalent influenza virus vaccine, without preservatives, administered in a 0.5 mL dose via intramuscular injection.
This code specifically reports IIV4 (Inactivated Influenza Vaccine, Quadrivalent) that protects against four influenza virus strains. It is commonly used for patients 6 months of age and older and is administered most often in the deltoid muscle.
Accurate reporting of CPT 90686 ensures correct claim processing, proper documentation, and fewer payer disputes during preventive care encounters.
Clinical Scenarios for CPT Code 90686
Followings are the clinical examples when CPT Code 90686 is applied:
An OB/GYN patient who is pregnant
During regular prenatal examinations, physicians commonly recommend a preservative-free quadrivalent influenza vaccine to protect both the mother and fetus. The Clinical Procedures Code 90686 is essential when administered intramuscularly and adequately documented.
Pediatric Patient With Egg Allergy
Children who have been diagnosed with egg allergies are routinely given quadrivalent flu shots that are free of preservatives. When administered intramuscularly with guardian consent, CPT 90686 is the appropriate vaccine product code.
Community or Senior Flu Clinics
Clinics hosting flu-shot events at senior centers often administer preservative-free quadrivalent vaccines. Even in outreach settings, CPT 90686 remains applicable when the product meets code requirements.
Does CPT Code 90686 Require a Modifier
CPT 90686 itself does not always require a modifier, but modifiers may be necessary depending on payer rules, patient eligibility, or vaccine sourcing, especially under VFC or Medicaid programs.
Modifiers Commonly Used With CPT Code 90686
Modifier 25
Used on the E/M code, not the vaccine code, when a significant, separately identifiable office visit occurs on the same date as the flu shot.
Modifier 59
Applied when distinct vaccination services are provided during the same encounter to avoid bundling issues.
Modifier 76
Used when the same provider repeats the vaccine due to a documented administration failure on the same day.
Modifier 77
Used when a different provider repeats the vaccine administration on the same date of service.
Modifier 95
Rarely applicable; only used if payer policy supports telehealth-based counseling related to the vaccination.
Modifier SL
Required when the vaccine is state-supplied (VFC or Medicaid). Failure to use SL is a frequent audit trigger.
CPT Code 90686 Billing & Reimbursement Guidelines
Establish Medical Necessity
Although influenza vaccines are preventive, payers may still request documentation showing appropriate administration and diagnosis linkage.
Ensure Complete Documentation
Always document:
Vaccine name and manufacturer
Lot number and expiration date
Route (intramuscular) and site
Date of administration
Patient consent
Use the appropriate Administrative Coding
Administration is not given in the CPT 90686. Pair it correctly:
Administration Code
Scenario
90460
Counseling provided (under 18)
90471
No counseling (18+)
90472
Additional vaccines
Manufacturer Brands Associated With CPT Code 90686
Common products billed under CPT 90686 include:
Fluarix Quadrivalent – GlaxoSmithKline
FluLaval Quadrivalent – GlaxoSmithKline
Fluzone Quadrivalent – Sanofi Pasteur
Matching the correct brand to the CPT code reduces payer scrutiny and denials.
When to Use CPT Code 90686
Use this code when:
The vaccine is quadrivalent
It is preservative-free
The dose is 0.5 mL
Administered intramuscularly
The patient is 6 months or older
When NOT to Use CPT Code 90686
Do not use CPT 90686 for:
High-dose vaccines (90662)
Adjuvanted vaccines (90653)
Intranasal vaccines (90660)
Pediatric 0.25 mL doses (90685 / 90687)
Preservative-containing vaccines (90688)
Common Denials Related to CPT Code 90686
Frequent denial reasons include:
Missing administration code
Incorrect or missing SL modifier
Absent diagnosis code Z23
Invalid or missing NDC
Age/dose mismatch
Billing state-supplied vaccines to payers
These issues are frequently seen in practices managing high vaccine volumes and often fall under vaccine billing claim denials during flu season.
How to Prevent CPT 90686 Claim Denials
Always pair with the correct admin code
Use Z23 consistently
Report the correct NDC for the dose administered
Apply Modifier SL when required
Never bill payers for free/state-supplied vaccines
Conclusion
After reviewing countless flu vaccine claims across primary care, pediatrics, OB/GYN, and community clinics, one thing is clear: understanding CPT Code 90686 goes far beyond knowing its definition. Practices that take the time to apply the code correctly, pairing it with the right administration code, diagnosis, modifier, and documentation, consistently see fewer denials and faster payments. Those that don’t often discover problems only after revenue has already slipped away.
From my experience, the most successful teams treat flu vaccine billing as a system, not a single code. When staff are trained, documentation is complete, and payer rules are respected, CPT 90686 becomes one of the cleanest and most reliable preventive-service claims to submit. If there’s one takeaway, it’s this: mastering the details today saves hours of rework, lost revenue, and frustration tomorrow, and that’s what sustainable medical billing is really about.
FAQs
What is CPT Code 90686?
CPT Code 90686 represents a quadrivalent, preservative-free influenza vaccine administered by intramuscular injection in a 0.5 mL dose. It is commonly used for patients 6 months of age and older during flu season.
What is the correct CPT code for a flu vaccine?
The type, dose, age group, and formulation of the flu vaccine all affect which CPT code is correct. 90686 (quadrivalent, preservative-free), 90688 (quadrivalent with preservative), and 90662 (high-dose for seniors) are all common examples.
Does CPT Code 90686 need a modifier?
CPT 90686 does not always require a modifier, but modifiers may be needed in certain situations. For example, Modifier SL is required for state-supplied vaccines, and Modifier 25 may apply to a separately billed E/M service (on the E/M code, not 90686).
Is CPT Code 90686 covered by Medicare?
Yes. As a preventative service, Medicare Part B usually pays for flu shots, which are CPT 90686. When billed correctly, patients usually don’t have to pay anything or have a deductible.
Is CPT Code 90686 approved by the FDA?
CPT codes individually are not FDA-approved; however, the influenza vaccines billed under CPT 90686 are accepted or authorized by the Food and Drug Administration (FDA). Only FDA-approved vaccine products should be used and documented.
Are the hepatitis A and B vaccines free of cost?
Hepatitis A and B vaccines may be free or low-cost when offered through public health programs, employer programs, or vaccination coverage plans. Coverage varies by the patient’s insurance, eligibility, and whether the vaccine is state-supplied and covered under preventive benefits.