Macrocytic anemia ICD-10 coding fails in real practice for one simple reason: coders look at the MCV and stop thinking.
An MCV above 100 fL appears in the lab panel, and the claim receives a generic anemia code without investigating why the red blood cells are enlarged. This shortcut creates confusion between D53.9 (nutritional anemia unspecified), D51.x (vitamin B12 deficiency anemia), and D64.9 (anemia unspecified)—three codes that represent very different clinical realities in the ICD-10-CM system.
Payers do not reimburse based on red blood cell size. They reimburse based on documented etiology.
When anemia codes fail to reflect the cause, claims face:
Downcoding
Medical review
Documentation queries
Audit flags
Underpayments
Denials that appear “mysterious” to billing teams
This guide connects hematology basics, ICD-10 rules, and payer behavior into one practical framework you can use on real charts.
Audience: Medical coders, billers, CDI specialists, and providers who want anemia claims to pass payer review the first time.
Why Macrocytic Anemia Coding Is Commonly Incorrect
The root problem is lab-driven coding instead of documentation-driven coding.
Example 4 MCV high, workup pending → D53.9 (temporary)
Why This Matters for Revenue
Specific anemia codes:
Reduce denials
Reduce documentation queries
Improve payer trust
Protect audits
Increase clean claim rates
Vague anemia coding does the opposite.
CDI and Provider Education Opportunity
Providers often document:
“Macrocytic anemia”
That phrase is not enough.
CDI teams should query for:
B12?
Folate?
Chronic disease link?
Conclusion
Macrocytic anemia is a lab observation. ICD-10 coding requires a clinical cause. When coders and providers align documentation with etiology, anemia claims pass payer review smoothly. When they don’t, D53.9 and D64.9 quietly drain revenue. Accurate macrocytic anemia coding is not about memorizing codes. It is about following the documentation trail to the cause.
Elevated ALT and AST levels show up in routine panels for patients with no pain, no jaundice, and no prior liver diagnosis. Multiple perspectives matter at this point because the clinical meaning (possible hepatocellular injury), the documentation burden (what the provider must state), and the billing risk (what the payer accepts) pull in different directions. Clear coding starts with one fact: ICD-10-CM does not code the word “transaminitis.” It codes the measurable finding. This blog focuses on USA-based ICD-10-CM workflows and uses the code that payers and code sets align with for isolated ALT/AST elevation: R74.01.
What “Transaminitis” Means in Clinical Documentation
Multiple perspectives matter because “transaminitis” functions as shorthand in clinical speech, not as a diagnosis label in ICD-10-CM. Transaminitis refers to elevated transaminase enzymes in blood testing, primarily:
ALT (alanine aminotransferase)
AST (aspartate aminotransferase)
ALT and AST live inside cells. Hepatocellular irritation or injury increases membrane leakage, raising serum levels. ALT tracks liver injury more directly than AST, since AST rises with liver injury and non-hepatic injury such as skeletal muscle disorders. Clinical references describe severity bands using multiples of the upper limit of normal (ULN), such as <2× ULN, 2–5× ULN, 5–15× ULN, and>15× ULN, with different diagnostic urgency at higher tiers.
A cause-based evaluation often starts with pattern recognition and risk review. Hepatology education materials emphasize historical factors like alcohol intake, medication lists, herbal products, viral hepatitis risk, metabolic risk, and physical signs of chronic liver disease.
Why ICD-10 Does Not List “Transaminitis” as a Code Title
Multiple perspectives matter because ICD-10-CM prioritizes classified findings and diagnoses, not informal clinical terms. Transaminitis describes a lab pattern, not an etiology. ICD-10-CM places that pattern under abnormal clinical and laboratory findings, which is why the correct code uses measurable language.
The practical result: providers search the code set for “transaminitis,” pick a nearby “abnormal enzyme” option, and end up with a code that does not defend liver-specific medical necessity.
The Correct ICD-10-CM Code for Transaminitis
Multiple perspectives matter because the “right” code depends on the level of certainty. A confirmed disease needs a disease code. An isolated lab abnormality needs an abnormal-finding code.
R74.01 – Elevation of liver transaminase levels is the ICD-10-CM code that matches elevated ALT/AST when a definitive liver diagnosis has not been established.
Coding teams see R74.01 used to support:
Repeat hepatic function panels
hepatitis serologies
iron studies
abdominal ultrasound orders
follow-up E/M for trend review
ICD-10-CM index entries show R74.01 as the destination for “elevation (ALT).”
Why R74.01 Gets Denials Even When It Is Correct
Multiple perspectives matter because a correct code still fails when documentation misses 1 of the payer-facing elements: severity, context, or plan.
Claims reviewers often see “elevated LFTs” in the assessment with no ALT/AST numbers. A chart without values weakens the link between abnormal findings and follow-up testing.
Denial trigger 2: no assessment language that matches R74.01
R74.01 describes elevated liver transaminases. Notes that focus only on “abnormal liver function,” “elevated enzymes,” or “abnormal labs” without naming ALT/AST invite code drift.
Denial trigger 3: plan lacksa medical-necessity bridge
Orders like ultrasound, hepatitis B testing, hepatitis C testing, or medication changes need a sentence that connects the abnormality to the plan.
Denial trigger 4: code never transitions to the diagnosis
R74.01 is not a permanent label once fatty liver disease, hepatitis, alcoholic liver disease, drug-induced injury, or other diagnoses become established.
ICD-10-CM guidance states symptom/sign codes are acceptable when a related definitive diagnosis has not been established. The same guidance discourages coding symptoms as “extra” once the definitive diagnosis exists and the symptom is integral to it.
R74.01 vs R89.0: Right Choice
Multiple perspectives matter because both codes mention “abnormal enzymes,” but they describe different specimen contexts.
R74.01 (liver blood chemistry focus)
Targets elevated liver transaminases
supports liver-focused workups
R89.0 (non-blood, non-liver specimen focus)
R89.0 — Abnormal level of enzymes in specimens from other organs, systems,, and tissues is intended for abnormal enzyme findings in specimens outside the “blood without diagnosis” section, such as synovial fluid or other tissue specimens, ns depending on the clinical scenario.
R89.0 reduces clarity for a payer reviewing a liver enzyme workup because it does not explicitly describe ALT/AST elevation in serum.
“Is R74.01 Billable?” and What Billers Actually Need to Know
Multiple perspectives matter because “billable” means “valid code,” while reimbursement depends on coverage rules and documentation quality.
R74.01 is a specific, billable ICD-10-CM diagnosis code. Payment still depends on:
the billed service (E/M level, lab panel, imaging CPT)
Multiple perspectives matter because inpatient “principal diagnosis” rules differ from outpatient “first-listed diagnosis” rules, and payer audits often focus on diagnosis sequencing logic.
ICD-10-CM guidance states that codes that describe signs and symptoms are acceptable for reporting when a related definitive diagnosis has not been established. That guidance supports R74.01 as first-listed when elevated transaminases represent the reason for the visit, and no diagnosis has been confirmed.
R74.01 becomes weaker as first-listed once documentation identifies an established etiology that has its own code. A confirmed condition should sequence ahead of the abnormal finding
Clinical Causes Where R74.01 is Not a Choice
Multiple perspectives matter because coders need cause categories that predict which diagnosis code will replace R74.01. Primary care literature lists common etiologies for mildly elevated transaminases, including NAFLD and alcohol-related liver disease, with other causes such as drug-induced liver injury, hepatitis B, hepatitis C, hemochromatosis, autoimmune hepatitis, and Wilson disease. Extrahepatic causes include thyroid disorders, celiac disease, hemolysis, and muscle disorders.
A practical way to document cause workup uses 4 buckets:
“Elevated ALT and AST on labs dated //____, ALT ___ U/L, AST ___ U/L.”
“Assessment: elevation of liver transaminases without established etiology.”
“Plan: repeat hepatic panel in ___ weeks, order hepatitis B testing and hepatitis C testing, order ultrasound, review medication exposures.”
Phrases that increase audit friction
“Rule out liver disease” without a defined plan.
“Abnormal labs” with no enzyme names and no values
“Transaminitis” with no link to ALT/AST
ICD-10-CM guidance supports coding to the level of certainty known for the encounter. Documentation that states uncertainty plus an action plan fits that rule.
Coding Measures That Reduce Denials
Multiple perspectives matter because coding decisions are not clinical guesses. Coding follows ca ertainty level.
Step 1: Confirm the finding
ALT and AST are listed in the record with values
Step 2: Check for an established diagnosis
imaging-confirmed fatty liver
documented viral hepatitis diagnosis
documented alcohol-associated liver disease
documented drug-induced liver injury
Step 3: Assign the code that matches certainty
no diagnosis established → R74.01
diagnosis established → assign the diagnosis code and stop leading with R74.01
Step 4: Update the problem list and claim sequencing
R74.01 was removed or moved behind the definitive diagnosis once confirmed
Real-World Example With Proper Sequencing
Multiple perspectives matter because examples show how documentation and coding move together.
Scenario
A 52-year-old patient reviews routine labs. ALT = 145 U/L. AST = 118 U/L. No prior liver disease diagnosis exists. Fatigue appears in ROS. Alcohol intake documented as 2–3 drinks on weekends. The medication list includes a statin and acetaminophen PRN.
Provider documentation (assessment)
“Elevation of liver transaminases without established etiology. ALT 145 U/L, AST 118 U/L.”
Provider documentation (plan)
“Repeat hepatic function panel in 4 weeks.”
“Order hepatitis B surface antigen and hepatitis C antibody.”
“Order RUQ ultrasound.”
“Review acetaminophen dosing limits and supplement exposures.”
Coding
First-listed diagnosis for that problem-focused visit: R74.01
Add secondary codes based on documented conditions that affect care that day, such as obesity or alcohol use disorder, only if documented and addressed.
A follow-up visit after an ultrasound showing fatty infiltration should switch away from R74.01 and use the confirmed diagnosis code that matches the imaging and provider assessment.
Reimbursement Guidelines
Multiple perspectives matter because code validity does not equal coverage approval.
R74.01 supports medical necessity for workups that match liver enzyme elevation. Clinical evaluation references describe structured approaches to abnormal liver enzymes that start with history, exam, and targeted testing.
R74.01 does not justify unrelated services. A claim with R74.01 paired to unrelated imaging or unrelated specialty referrals often triggers edits.
Major ICD-10 Coding Mistakes With Transaminitis
Multiple perspectives matter because the same mistake repeats across practices.
Mistake 1: Using a non-specific enzyme code instead of R74.01 for ALT/AST elevation
Mistake 2: Using R74.01 after a definitive diagnosis is documented
Mistake 3: Missing ALT/AST values in the note
Mistake 4: Listing R74.01 with a plan that does not address liver enzymes
Mistake 5: Treating “transaminitis” as a diagnosis label rather than an abnormal finding
ICD-10-CM guidance explicitly supports symptom/sign reporting only until confirmation of a related definitive diagnosis.
How Long Does R74.01 Stay Appropriate?
Multiple perspectives matter because monitoring is clinical, while coding is certainty-based.
R74.01 stays appropriate across repeated visits only while the record still reflects:
ALT/AST elevation present
etiology not established
workup in progress or monitoring required
Persistent elevation drives more structured evaluation pathways in clinical guidance, with NAFLD and alcohol-related liver disease listed as common causes in outpatient care. A diagnosis established during that workup should replace R74.01 as the leading code.
Conclusion
Multiple perspectives matter because transaminitis coding sits at the intersection of clinical uncertainty and payer certainty. Elevated ALT and AST levels require documentation that states the finding, quantifies it, and explains the plan.
R74.01 is the correct ICD-10-CM code for elevation of liver transaminase levels when no definitive liver diagnosis exists. Clean documentation protects reimbursement, supports medical necessity for workups, and reduces audit exposure. Code transitions complete the cycle once a confirmed diagnosis appears in the record.
FAQs
What is the ICD-10-CM code for transaminitis?
R74.01 matches the elevation of liver transaminase levels in ICD-10-CM.
Is R74.01 a billable code?
R74.01 is a billable ICD-10-CM diagnosis code.
Can R74.01 be first-listed?
R74.01 fits the first-listed use when elevated transaminases drive the visit, and no definitive diagnosis has been established. ICD-10-CM guidance supports symptom/sign code reporting under that condition.
What causes elevated ALT and AST?
Common causes cited in primary care literature include NAFLD and alcohol-related liver disease, with other causes such as viral hepatitis, drug-induced liver injury, and hereditary disorders.
When should R74.01 be replaced?
A confirmed diagnosis code should replace R74.01 once the provider documents a definitive etiology that has its own ICD-10-CM code.
Treating patients takes time. Coding weakness correctly takes discipline. The symptom sounds simple, yet “weakness” becomes a denial magnet when the documentation does not match the ICD-10 code choice. Many practices bounce between M62.81 (generalized muscle weakness), R53.1 (weakness), and other symptom codes without a consistent rule set. The result shows up in three places: rejected claims, audit exposure, and delayed reimbursement.
Generalized weakness coding succeeds when one chain stays intact:
Break one link, and the payer treats the service as unsupported, even when the care was clinically appropriate. This guide explains what “generalized weakness” means, how to select the M62.81 diagnosis code correctly, when to avoid it, and how to document it in a way that survives payer review.
What “Generalized Weakness” Means in Clinical Documentation
Generalized weakness describes strength loss across multiple muscle groups with a measurable impact on function. The symptom does not follow a single limb pattern (only right arm, only left leg) and does not match one nerve distribution.
Generalized weakness shows up in documentation as functional loss, such as:
Difficulty rising from a chair without arm support
Trouble climbing stairs due to proximal leg weakness
Reduced walking tolerance with instability
Decline in lifting/carrying capacity
Recurrent falls are linked to loss of strength and balance
Weakness vs Fatigue vs Deconditioning
Coding accuracy starts by separating three commonly mixed concepts.
Typical documentation: objective deficits on strength testing, functional impairment
Better code: M62.81 when weakness is generalized
Deconditioning
Primary issue: performance decline after inactivity, illness, or hospitalization
Documentation must still show objective weakness/functional decline if M62.81 is used.
Deconditioning often supports medical necessity for therapy when measured deficits exist.
Weakness is not a final diagnosis. Weakness is a clinical finding that requires evaluation, a functional plan, and clear coding logic.
ICD-10 Code for Generalized Weakness: What M62.81 Represents
ICD-10-CM M62.81 = Generalized muscle weakness.
Use M62.81 when documentation supports:
Strength reduction across more than one anatomical region or muscle group
Functional impairment that affects daily activities or mobility
Exam findings that support the assessment (manual muscle testing, functional testing, gait/balance observations)
M62.81: Diagnosis code or symptom code?
M62.81 functions as a measurable impairment code. The payer sees it as “documented functional weakness” rather than a disease label. That distinction matters:
Primary diagnosis use: generalized muscle weakness is the chief reason for the visit, evaluation, or therapy plan, and the underlying etiology is still under workup or not established in the record.
Secondary diagnosis use: a confirmed condition exists, and generalized weakness represents a documented impairment that affects function and drives the treatment plan.
Repeated long-term billing with only M62.81 and no evolving assessment raises payer suspicion. Claims pass when the record shows progression: updated findings, measurable outcomes, and etiology-focused evaluation when appropriate.
When to Use ICD-10 Code M62.81?
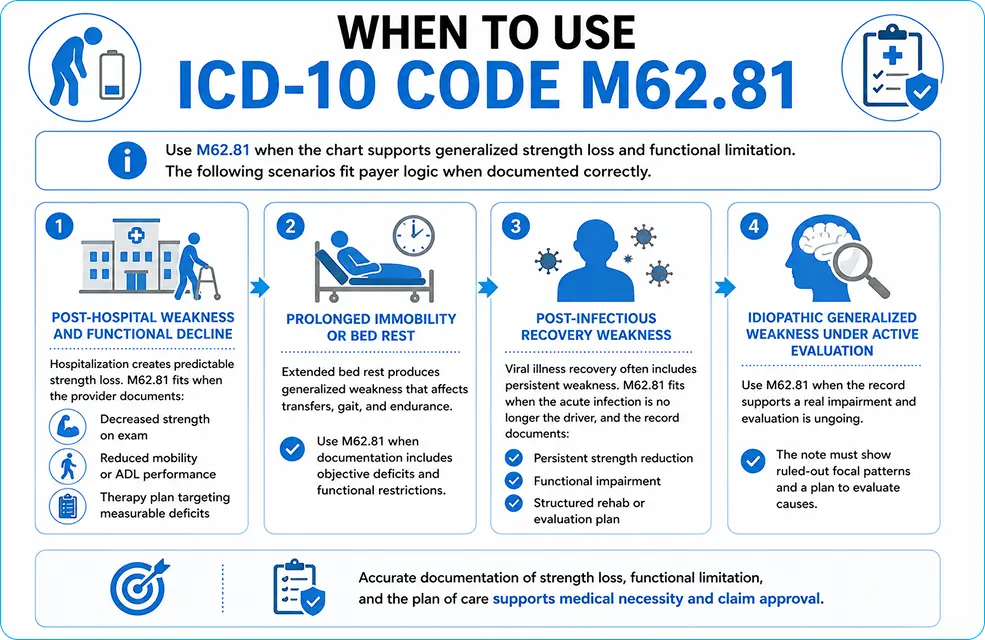
Use M62.81 when the chart supports generalized strength loss and functional limitation. The following scenarios fit payer logic when documented correctly.
1) Post-hospital weakness and functional decline
Hospitalization creates predictable strength loss. M62.81 fits when the provider documents:
decreased strength on exam
reduced mobility or ADL performance
therapy plan targeting measurable deficits
2) Prolonged immobility or bed rest
Extended bed rest produces generalized weakness that affects transfers, gait, and endurance. Use M62.81 when documentation includes objective deficits and functional restrictions.
3) Post-infectious recovery weakness
Viral illness recovery often includes persistent weakness. M62.81 fits when the acute infection is no longer the driver, and the record documents:
persistent strength reduction
functional impairment
structured rehab or evaluation plan
4) Idiopathic generalized weakness under active evaluation
Use M62.81 when the record supports a real impairment and evaluation is ongoing. The note must show ruled-out focal patterns and a plan to evaluate causes.
When NOT to Use ICD-10 Code M62.81
M62.81 fails when the record describes “weakness” in words but does not prove muscle weakness in findings.
Do not use M62.81 for a fatigue-only complaint.s
Fatigue without objective weakness belongs under fatigue/malaise coding, not generalized muscle weakness.
Do not use M62.81 for localized weakness
Weakness in one limb or one side requires more specific coding. Examples:
right arm weakness only
left leg weakness only
facial weakness
isolated hand grip weakness
Localized patterns demand localized codes or neurologic etiologies when present.
Do not use M62.81 for neurologic deficits with a clear etiology
Stroke-related hemiparesis, hemiplegia, neuropathy, and other neurologic deficits require neurologic diagnosis coding. Coding M62.81 instead of neurologic diagnoses creates a medical necessity mismatch.
Do not use M62.81 when sarcopenia is confirmed.
M62.84 (sarcopenia) represents age-related muscle loss. Confirmed sarcopenia must be coded as sarcopenia, not replaced by generalized weakness.
ICD-10 Exclusion Logic: What Not to Report With M62.81
Coding compliance requires attention to ICD-10 “Excludes” notes.
Excludes1 (do not code together)
Excludes1 means “mutually exclusive.” Conditions with distinct definitions must not be reported with M62.81 when the excludes rule applies. Examples commonly listed in the category include:
alcoholic myopathy
drug-induced myopathy
muscle cramps/spasms
myalgia
stiff-person syndrome
Excludes2 (both can exist, both require documentation)
Excludes2 means both conditions can exist at the same time, and both codes can be used when each is supported in the record. Dual coding requires separate supporting documentation for each condition.
M62.81 vs R53.1: How to Choose the Correct Weakness Code
Use M62.81 when the record documents measurable strength reduction and functional impairment.
Use R53.1 when the record documents generalized weakness as a constitutional symptom without objective muscle weakness findings, or when the note supports “debility/asthenia” more than strength loss.
Payer behavior: M62.81 aligns better with therapy plans because therapy notes usually contain objective deficits. R53.1 often triggers “symptom-only” scrutiny when paired with extensive therapy without functional testing in the record.
M62.81 vs M62.84 Sarcopenia: What Changes in Documentation
Sarcopenia (M62.84) requires documentation consistent with age-related muscle mass and strength decline. Coding must reflect that diagnosis when the clinician confirms it.
Do not “water down” confirmed sarcopenia into M62.81. Payers and auditors look for correct diagnostic specificity when the provider identifies a defined condition.
Other Codes Often Confused With M62.81
Limb-specific weakness patterns
A limb-specific pattern demands specific coding rather than generalized weakness. The chart should answer:
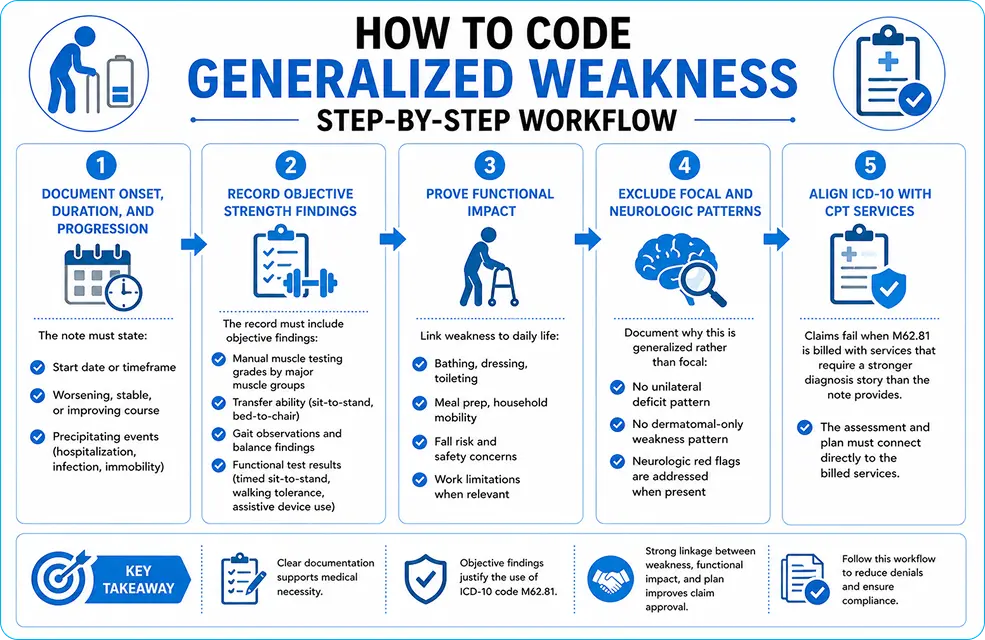
The record must include objective findings, not only patient statements. Examples:
manual muscle testing grades by major muscle groups
transfer ability (sit-to-stand, bed-to-chair)
gait observations and balance findings
functional test results (timed sit-to-stand, walking tolerance, assistive device use)
Step 3: Prove functional impact
Link weakness to daily life:
bathing, dressing, toileting
meal prep, household mobility
fall risk and safety concerns
work limitations when relevant
Step 4: Exclude focal and neurologic patterns
Document why this is generalized rather than focal:
no unilateral deficit pattern
no dermatomal-only weakness pattern. Neurologic red flags are addressed when present
Step 5: Align ICD-10 with CPT services
Claims fail when M62.81 is billed with services that require a stronger diagnosis story than the note provides. The assessment and plan must connect directly to the billed services.
Required Documentation Elements for M62.81
A payer-ready note includes:
Chief complaint: generalized weakness with functional limitation
Etiology workup: documented evaluation steps when appropriate
Sample documentation statements that reduce denials
Use direct, measurable language:
“Strength reduced across bilateral hip flexors and knee extensors with impaired sit-to-stand transfers; patient requires arm support to rise from chair.”
“Generalized weakness limits stair climbing; patient reports two falls in 30 daysgait t is unsteady with reduced step height.”
“Post-hospital functional decline with decreased strength in multiple muscle groups; ADL assistance required for bathing and dressing.”
Is ICD-10 Code M62.81 Billable?
Yes. M62.81 is a billable ICD-10-CM code. Reimbursement depends on medical necessity and documentation quality, not the billable status alone.
Denial patterns appear when:
Functional impairment is missing from the record
Objective strength findings are absent
Repeated use continues without updated findings or diagnostic clarification
ICD-10 does not support the intensity/type of billed services
Medicare and Payer Perspective on M62.81
Medicare and commercial payers expect:
Objective findings supporting weakness
functional limitation supporting treatment
progression tracking when services continue over time
diagnosis refinement when evaluation identifies a cause
Common payer red flags:
“weakness” was stated only in the subjective section
No strength testing was documented
therapy billed without functional goals tied to deficits
M62.81 was used repeatedly without an updated assessment
Common Claim Denials Linked to M62.81
Denials typically tie to documentation gaps rather than the code itself:
Missing objective strength findings
Missing ADL or mobility impact
Weak plan-of-care connection to billed services
Non-specific coding when a specific cause is documented elsewhere in the record
No progress reporting for continued therapy
Denial prevention comes from structured charting, consistent reassessment, and CPT-to-diagnosis alignment.
CPT Codes Commonly Billed With M62.81
Common CPT families that pair with generalized weakness claims:
E/M services for evaluation and medical decision making
Physical therapy evaluation and re-evaluation codes
Therapeutic exercise and neuromuscular re-education codes
Gait training and functional performance testing codes
Payer review focuses on one question: Do the documented deficits justify the billed services? The note must answer that question directly.
How Long to Use M62.81 Without Raising Audit Risk
Short-term use fits the evaluation and early treatment phases. Continued use requires:
updated objective findings
measurable functional progress or documented barriers
diagnosis refinement when a cause becomes clear
Long-term repeated use with no updated findings creates avoidable audit exposure.
Special Scenarios
Post-COVID generalized weakness
Documentation must be separate:
active infection vs post-infectious recovery
Objective strength deficits
functional impairment and safety concerns
structured plan with measured progress
Weakness in older adults
Older patients require clear separation between:
generalized weakness (M62.81)
confirmed sarcopenia (M62.84)
Neurologic causes of weakness when present Fall risk documentation strengthens medical necessity when accurate and specific.
Coding Mistakes That Trigger Denials
Coding fatigue as muscle weakness without objective findings
Using M62.81 for one-limb or one-side weakness
Ignoring exclusion logic and reporting conflicting codes
Failing to code the confirmed underlying cause when documented
Submitting therapy claims without functional goals and reassessment data
Conclusion
Recap: M62.81 succeeds when generalized muscle weakness is proven with objective findings and functional impact. Evidence in the chart: strength deficits across multiple muscle groups, ADL limits, gait/transfer issues, fall risk factors, and reassessment data. Steps: document onset/progression, test strength, prove functional impairment, exclude focal/neurologic patterns, align ICD-10 with CPT. Takeaway: clean generalized weakness coding protects reimbursement, reduces denials, and keeps documentation audit-ready.
FAQs
What is the ICD-10 code for generalized weakness?
M62.81 reports generalized muscle weakness when objective findings support multi-muscle-group strength loss.
Yes, when generalized muscle weakness is the chief reason for evaluation or treatment, and the record documents objective deficits and functional impairment.
Will Medicare reimburse claims with M62.81?
Yes, when documentation supports medical necessity and CPT alignment.
What documentation is required for M62.81?
Objective strength findings, functional limitation, symptom duration/progression, assessment, and a plan tied to measurable deficits.
Does M62.81 trigger denials?
Yes, when objective findings and functional impact are missing, or when the code is used repeatedly without an updated assessment.
Can CPT 43239 be billed multiple times for different biopsy sites?
CPT 43239 is typically reported once per session, even if multiple biopsy samples are taken from different areas of the upper GI tract. The code represents the overall procedure, not the number of samples. However, if distinct procedures are performed at separate anatomical sites with clear documentation, modifiers like 59 may be required to indicate separate services.
Medical coding errors in hematology often start with vocabulary. Clinical notes use phrases such as “neutrophilic leukocytosis,” “neutrophilia,” and “leukemoid reaction.” Each phrase points to a different clinical concept, and ICD-10-CM expects the coder to select a code that matches the documented diagnosis, not the lab narrative.
Claim denials follow predictable patterns. A payer sees an elevated WBC. The diagnosis code stays nonspecific across repeated encounters. Documentation fails to connect the abnormal count to an assessed condition. The record looks incomplete. Rework increases. Payment slows.
Coders need a repeatable method. A repeatable method starts with 3 anchors:
Clinical meaning: What the term describes in blood physiology.
ICD-10-CM structure: Which D72.82 subcode fits the documented diagnosis?
Guideline compliance: What ICD-10-CM allows based on documentation at the time of the encounter.
This article builds on that method.
Neutrophilic Leukocytosis: The Clinical Definition for Coders
Neutrophilic leukocytosis means an abnormally high number of neutrophils in the blood. The phrase often appears in assessment sections, ED summaries, inpatient progress notes, and discharge diagnoses.
Neutrophils rise during immune and stress responses. Common triggers include bacterial infections, tissue injury, inflammation, corticosteroid exposure, and physiologic stress states such as surgery and trauma. Merck Manual describes neutrophilic leukocytosis as a high neutrophil count and lists infections and injuries among common drivers.
Coders should treat “neutrophilic leukocytosis” as a clinical description that needs translation into ICD-10-CM terms.
Neutrophilia is defined by an increased absolute neutrophil count (ANC) above the expected reference range. StatPearls describes neutrophilia as the most common leukocytosis type and gives a commonly used adult threshold around >7,700 neutrophils/µL (roughly 2 standard deviations above the mean).
A standard ANC formula multiplies WBC by the sum of neutrophil and band percentages, then divides by 100.
Example with consistent units:
WBC: 14.0 ×10³/µL
Neutrophils: 82%
Bands: 3%
ANC: 14.0 × (82 + 3) / 100 = 11.9 ×10³/µL
That ANC supports a neutrophil-driven leukocytosis.
Coding still requires documentation alignment. ANC supports a query. ANC does not replace a provider diagnosis statement in ICD-10-CM coding.
Leukemoid Reaction: A Pattern that Impacts Code Selection
A leukemoid reaction is not “high WBC” in a generic sense. The Merck Manual describes a leukemoid reaction as a neutrophil count >50,000/µL not caused by malignant transformation of a hematopoietic stem cell. That definition matters for coding because ICD-10-CM assigns a dedicated code to leukemoid reaction.
Leukemoid reaction also overlaps with oncology differentials. Chronic neutrophilic leukemia and chronic myeloid leukemia can mimic benign neutrophilia, which is why documentation clarity matters.
ICD-10-CM Simplified
ICD-10-CM does not provide a billable code titled “neutrophilic leukocytosis.” ICD-10-CM provides a category for elevated WBC and billable subcodes under it. D72.82 “Elevated white blood cell count” is a non-billable header category.
Billable selection happens at the subcode level.
Key codes used in this documentation space:
D72.823 – Leukemoid reaction
D72.828 – Other elevated white blood cell count
D72.829 – Elevated white blood cell count, unspecified
A frequent error involves D72.819. D72.819 is “Decreased white blood cell count, unspecified.” It belongs to decreased WBC logic, not elevated neutrophils.
Documentation Rule that Protects Audits
ICD-10-CM coding guidelines state that diagnosis code assignment is based on the provider’s diagnostic statement that the condition exists. Code assignment is not based on the clinical criteria the provider used to establish the diagnosis. Conflicting documentation requires a provider query.
That guideline has direct implications:
A CBC that shows neutrophilia does not authorize a neutrophilia diagnosis code without provider documentation.
A note that states “leukocytosis” without subtype supports an unspecified elevated WBC code.
A chart that contains mixed terms (“leukocytosis” in one note, “leukemoid reaction” in another) requires reconciliation through query or clarified discharge diagnosis.
Choosing between D72.828 and D72.829
Coders typically face one operational decision more than any other: D72.828 vs D72.829.
Use D72.829 for documented leukocytosis without subtype
D72.829 fits documentation that states elevated WBC or leukocytosis with no specified cell-line driver.
Use cases include:
ED workup where the assessment lists “leukocytosis” and plans repeat CBC
Early inpatient day where the differential workup is pending
Outpatient follow-up note that lists “leukocytosis” without specifying neutrophilia, lymphocytosis, monocytosis, or bandemia
Use of D72.828 for Specified Elevated WBC Patterns
D72.828 covers “other elevated white blood cell count.” This code often becomes the most defensible option when the provider documents neutrophilia or neutrophilic leukocytosis, but the case does not meet leukemoid reaction criteria, and no narrower D72.82 subcode applies.
A tighter documentation phrase supports D72.828:
“Neutrophilia secondary to corticosteroid exposu..re”
“Reactive neutrophilia related to pneumoni..a”..
“Neutrophilic leukocytosis, monitor ANC tren..d”
A record that only contains lab values without a diagnostic statement supports a query, not an automatic shift from D72.829 to D72.828.
Selecting D72.823: Leukemoid Reaction Threshold
D72.823 is reserved for leukemoid reaction. That diagnosis implies an extreme neutrophil elevation pattern, commonly referenced as >50,000/µL neutrophils in clinical resources.
Coding triggers that support D72.823:
Provider documents “leukemoid react..ion”
Workup notes extreme leukocytosis with left shift and explicitly labels it leukemoid rea..ction
Discharge summary includes leukemoid reaction as a problem addressed
Documentation that says “rule out leukemia” does not justify leukemoid reaction by itself. Leukemoid reaction and leukemia are separate diagnostic categories. Merck’s definition explicitly distinguishes leukemoid reaction from malignant transformation.
4-Step Lab-to-Documentation Workflow
Step 1: Extract 3 CBC elements
Coders need values that show the pattern:
Total WBC
Neutrophil % and/or absolute neutrophils
Bands % (when reported)
Step 2: Convert the pattern into a question
Patterns do not equal diagnoses in ICD-10-CM. The pattern creates a query target.
Examples:
WBC 18.2 with ANC 14.7 → “Assessment includes neutrophilia?”
WBC 52.0 with left shift → “Assessment includes leukemoid reaction?”
Step 3: Anchor code selection to the provider statement
ICD-10-CM requires the provider’s statement for diagnosis code assignment.
Outcomes:
Provider documents “neutrophilia” → D72.828 fits when no narrower subcode applies.
Provider documents “leukocytosis” only → D72.829 fits.
Step 4: Update codes across the timeline of certainty
ICD-10-CM guidelines permit sign/symptom/unspecified use when information is insufficient, and they require coding to the certainty known at the encounter. A later clarified diagnosis supports code revision in subsequent encounters or on final billed diagnoses, based on facility policy and coding rules.
Mistakes that Trigger Denials in Neutrophilic Leukocytosis Coding
Denials in this area map to 3 documentation failures.
1) Unlinked abnormal finding
A claim lists D72.829, but the note lacks an assessed condition that explains evaluation intensity. Plans such as cultures, imaging, IV antibiotics, and repeat CBCs need a documented rationale tied to diagnoses such as pneumonia, pyelonephritis, cellulitis, or sepsis.
2) Subtype mismatch
The chart documents neutrophilia, bandemia, or leukemoid reaction, but the claim uses D72.829. Mismatch raises the question of why a specific documented diagnosis did not translate into a specific code.
3) Provider note conflict
One note labels leukemoid reaction. Another note labels simple leukocytosis. ICD-10-CM guidelines direct coders to query the provider when documentation conflicts.
Primary vs Secondary Diagnosis in Neutrophilic Leukocytosis
Sequencing depends on what drove the encounter.
Infection-driven workups
A diagnosis such as pneumonia, UTI, cellulitis, or sepsis often drives admission and treatment. Neutrophilia or leukocytosis functions as a severity marker or supporting finding.
Sequencing pattern:
Principal: infection diagnosis (when established)
Secondary: D72.828 or D72.829 (when documented as a condition evaluated/managed)
Medication-driven neutrophilia
Steroids and growth factors can elevate neutrophils. Documentation should name the medication exposure and the assessed blood count condition.
Secondary: D72.828 (documented neutrophilia) plus medication-related codes when applicable under payer and setting rules
A coding decision still hinges on provider documentation that the elevated neutrophils represented a condition addressed, not a silent lab abnormality.
Specialty-specific documentation cues
Emergency medicine and hospital medicine
ED and inpatient documentation often includes “leukocytosis” in MDM. A short query template reduces rework:
“CBC shows WBC __ and ANC __. Assessment lists leukocytosis. Diagnosis intended: leukocytosis unspecified vs neutrophilia vs leukemoid reaction?”
Hematology and oncology
Oncology charts include leukemia differentials. Leukemoid reaction explicitly excludes malignant transformation in standard definitions. Cancer coding requires confirmed malignancy diagnoses. Problem lists that say “concern for leukemia” need final diagnostic statements before malignancy code assignment.
Internal medicine and rheumatology
Chronic inflammation patterns can sustain neutrophilia. Documentation should name inflammatory drivers such as rheumatoid arthritis flares, inflammatory bowel disease activity, vasculitides, or chronic infections, plus the assessed leukocytosis type.
Realtime Coding Scenarios
Scenario 1: ED patient with bacterial pneumonia and neutrophilia
Documentation facts:
WBC 17.6
Neutrophils 86%
Provider documents “pneumonia” and “reactive neutrophilia.”
Coding outcome:
The pneumonia code sequenced first
D72.828 sequenced as an additional diagnosis due to documented neutrophilia pattern
Scenario 2: Steroid-associated neutrophilia in an outpatient visit
Diagnosis term captured: leukocytosis vs neutrophilia vs leukemoid reaction documented by the provider
CBC snapshot retained: WBC, differential, ANC values recorded in the coding abstraction
Documentation conflict resolved: queries sent when the problem list and assessment disagree.
Specificity used when available: D72.823 or D72.828 selected when documented; D72.829 reserved for insufficient specificity.
Wrong-code trap avoided: D72.819 remains a decreased WBC code, not a neutrophilia code
Conclusion
Neutrophilic leukocytosis coding becomes stable after the terminology is pinned to the ICD-10-CM structure and guideline rules. Provider-documented diagnoses determine code assignment. Unspecified codes remain valid when documentation is insufficient. Extreme neutrophil elevations labeled “leukemoid reaction” demand a dedicated code.
Accurate selection reduces rework, protects the record during audits, and aligns reimbursement with the documented severity of illness.
FAQs
What ICD-10-CM code fits leukocytosis with neutrophil predominance?
Provider-documented neutrophilia or neutrophilic leukocytosis often maps best to D72.828. Other elevated white blood cell counts when no narrower D72.82 subcode applies.
What code fits leukocytosis without a stated subtype?
D72.829 Elevated white blood cell count, unspecified fits when the record lacks enough detail for a more specific D72.82 subcode.
What code fits leukemoid reaction?
D72.823 Leukemoid reaction is the billable ICD-10-CM code.
Can coders assign neutrophilia codes based only on ANC?
ICD-10-CM guidelines state that the diagnosis code assignment is based on the provider’s diagnostic statement. ANC supports a query and supports medical record interpretation. ANC does not replace provider documentation for diagnosis coding.
What is the ICD-10-CM risk in using D72.819 for neutrophilia?
D72.819 is “Decreased white blood cell count, unspecified.” Using it for neutrophilia flips the meaning of the condition and creates medical necessity conflicts.
ICD-10 refers to the International Classification of Diseases, 10th Revision. Doctors and nurses often use this method to group medical conditions and treatments. This coding system makes it easier to correctly sort diagnoses, write clinical notes, and charge for medical services. Each code is very important for figuring out how to pay for medical diagnoses. It is very important to write down injuries in ICD-10 because it shows how bad the injury is and where it happened.
In dog bite cases, injuries must be classified correctly so that patients can get the best care, and the right amount of money can be paid back. Healthcare professionals use standardized coding and billing to keep accurate records, improve patient outcomes, and help with research and statistical analysis in the healthcare field.
What is ICD-10?
The ICD-10 medical coding system is always changing to make sure that health records are correct. A lot more diagnosis and procedure codes have been added since the US healthcare system switched from ICD-9 to ICD-10 in 2015. These changes make it easier to remember where the body is, what caused the injury, and how bad the illness is.
The 2026 ICD-10 updates are all about being more precise, keeping better track of information, and making medical histories easier to understand. Changes to how medical coding and billing work are meant to make documentation and healthcare data analytics even better.
Accurate coding is critical, as these ICD-10 revisions directly affect reimbursement and compliance.
ICD-10 External Cause Codes for Animal-Related Injuries
External causes of morbidity are used to explain how an injury occurred. Animal-related injuries fall into this category and include dog bite injuries from both nonvenomous animals and venomous animals. These codes document exposure to animate mechanical forces and help explain the injury mechanism and injury origin.
ICD-10 W-codes play a key role in the coding hierarchy and classification of animal injuries. They support clinical documentation, injury surveillance, and statistical injury tracking. Healthcare research depends on this data to analyze trends and improve patient safety.
What Is W54.0XXA?
The ICD-10 code for dog bite injuries that happen during a first encounter is W54.0XXA. This part explains what the code means, how it works, and when it should be used in real-life medical situations.
What does the code mean?
The ICD-10 code W54.0XXA means “bitten by dog, first time.” You can bill for healthcare diagnosis reimbursement with this ICD-10 code. After the switch to ICD-10, this code took the place of the ICD-9 code E906.0.
When medical documentation backs it up, the billable status means it can be reported on claims. It falls under exposure to animate mechanical forces and is used to describe the injury encountered during the initial treatment visit. Correct medical classification makes sure that billing and payment are done correctly.
Dog Bite ICD 10
Dog bite ICD-10 coding helps healthcare providers document animal-related injuries accurately for treatment, reporting, and reimbursement. The W54 category identifies injuries caused by dog bites and supports proper clinical documentation, injury classification, and medical billing workflows.
Infection Risk After a Dog Bite
Dog bite injuries carry a high risk of bacterial infection because animal saliva can transfer harmful microorganisms into soft tissue and open wounds. Deep puncture wounds, hand injuries, delayed treatment, and poor wound cleaning increase the risk of cellulitis, abscess formation, and tissue damage. Healthcare providers often evaluate tetanus immunization status, rabies exposure risk, and wound contamination during clinical assessment. Accurate documentation of infection risk supports proper ICD-10 coding, treatment planning, and medical necessity reporting.
W54.0 Explained
W54 is the external cause code category for dog bite injury. The code structure includes body part specificity, such as right hand, left hand, face, right leg, and left leg. It also includes encounter characters like initial encounter, subsequent encounter, and sequela.
These encounter characters work alongside S codes, which are injury nature codes. This code composition helps with billing, getting paid back, and making sure that the diagnosis and procedure match up. Knowing how ICD-10 is set up can help you avoid making mistakes when coding.
Use Cases
People often go to the emergency department for the first time to get treatment for dog bites, where accurate injury documentation and coding are critical. During visits to a healthcare provider, wound care, infection risk management, and injury severity assessment may all be done.
Follow-up care or treatment of sequelae conditions is often part of later visits. Medical records must clearly show what kind of treatment was given so that accurate reporting and payment can happen.
Coding Scenarios for Dog Bites
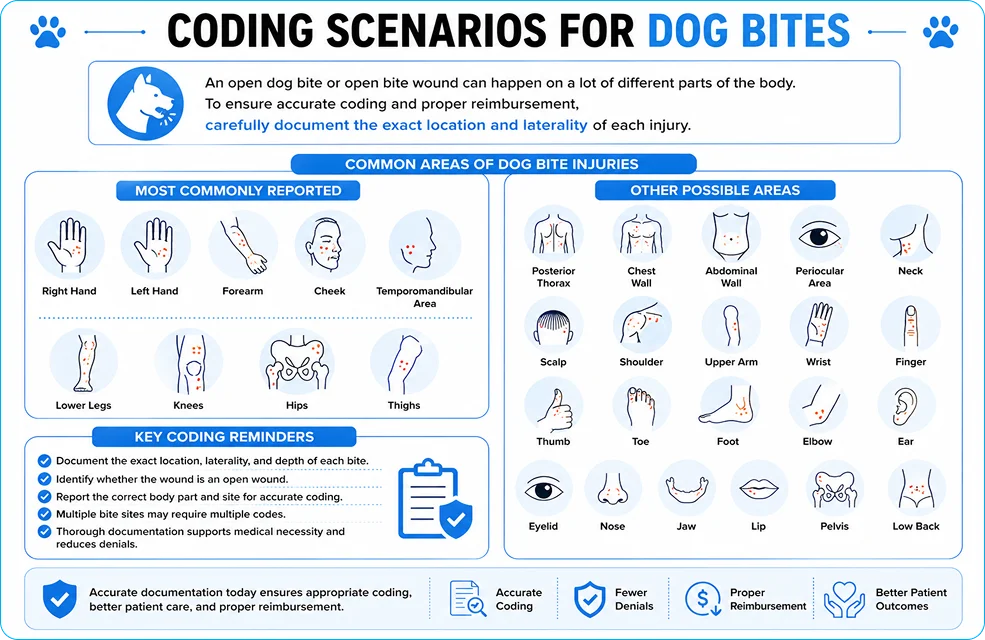
An open dog bite or open bite wound can happen on a lot of different parts of the body. Some common areas of injury are the right hand, left hand, forearm, cheek, and temporomandibular area. People often report injuries to their lower legs, knees, hips, and thighs.
In other cases, injuries to the posterior thorax, chest wall, abdominal wall, periocular area, neck, scalp, shoulder, upper arm, wrist, finger, thumb, toe, foot, elbow, ear, eyelid, nose, jaw, lip, pelvis, and low back are possible. To make sure that coding is correct, each location needs to be carefully documented.
Dog Bite ICD Coding With Respect to Body Parts
Dog bite ICD coding changes according to the injured body part, laterality, wound type, and encounter status. The dog bite itself is not enough for clean coding. The claim should show the actual injury first, such as an open bite of the right hand, left forearm, thigh, or lower leg. The external cause code W54.0XXA, “bitten by dog, initial encounter,” is added after the injury code to explain how the injury happened. ICD-10-CM official guidance also states that an external cause code should not be reported as the principal or first-listed diagnosis.
For active treatment, most dog bite encounters use the “A” seventh character for initial encounter. Follow-up care after active treatment uses “D”, and long-term effects use “S” for sequela. The provider note should clearly document the exact body part, right or left side, depth of wound, infection status, and whether the wound is open, superficial, puncture-type, or complicated.
Body Part
ICD-10-CM Code
Code Description
Right hand dog bite
S61.451A
Open bite of right hand, initial encounter
Left hand dog bite
S61.452A
Open bite of left hand, initial encounter
Left forearm dog bite
S51.852A
Open bite of left forearm, initial encounter
Right forearm dog bite
S51.851A
Open bite of right forearm, initial encounter
Left thigh dog bite
S71.152A
Open bite, left thigh, initial encounter
Right thigh dog bite
S71.151A
Open bite, right thigh, initial encounter
Left lower leg dog bite
S81.852A
Open bite, left lower leg, initial encounter
Right lower leg dog bite
S81.851A
Open bite, right lower leg, initial encounter
These body-part codes describe the injury site. W54.0XXA explains the cause: bitten by dog. Hand, forearm, thigh, and lower-leg open bite codes are listed under ICD-10-CM injury categories for open wounds of those regions.
ICD 10 Code for Dog Bite Right Hand
The ICD-10 code for dog bite right hand is S61.451A when the documentation supports an open bite of the right hand during active treatment. This code should be listed before W54.0XXA because the hand wound is the actual diagnosis, while the dog bite code explains the cause.
Right-hand dog bites need careful documentation because hand wounds have higher clinical concern due to tendons, joints, nerves, and infection risk. The note should mention whether the wound involves the palm, dorsum of hand, fingers, puncture injury, crush injury, cellulitis, abscess, or foreign material.
Left Hand Dog Bite ICD 10
The ICD-10 code for left hand dog bite is S61.452A for an open bite of the left hand, initial encounter. Use this code only when the provider clearly documents the left hand as the injured site. If the record says only “hand bite” without laterality, the claim loses specificity and may require an unspecified hand code instead.
For clean billing, the documentation should connect the wound to the dog bite event. A stronger note would say: “Open bite wound of left hand caused by dog bite, initial treatment provided.” That supports both the injury code and the external cause code.
Dog Bite Left Forearm ICD 10
The ICD-10 code for dog bite left forearm is S51.852A when the injury is documented as an open bite of the left forearm during the initial encounter. ICD-10 separates forearm wounds from hand, wrist, elbow, and upper arm wounds, so the provider’s exact anatomic wording matters.
A left forearm dog bite should not be coded as a hand wound, elbow wound, or unspecified arm wound unless the documentation supports that site. For claim accuracy, the note should identify the forearm area, wound type, laterality, and whether infection or deeper tissue involvement is present.
Dog Bite Right Forearm ICD 10
The ICD-10 code for dog bite right forearm is S51.851A for an open bite of the right forearm, initial encounter. This code fits when the bite is located between the elbow and wrist and the provider documents an open bite injury.
Right forearm bites need precise wording because coders must avoid mixing forearm wounds with wrist, hand, or elbow codes. If the bite is near the wrist but documented as forearm, S51.851A fits. If the provider documents wrist or hand involvement, a different code category may be needed.
Left Thigh Dog Bite ICD 10
The ICD-10 code for left thigh dog bite is S71.152A for an open bite of the left thigh, initial encounter. Thigh wounds fall under the hip and thigh injury category, not the lower-leg category.
Documentation should state “left thigh” clearly. Vague phrases like “left leg bite” are weaker because ICD-10 separates thigh, lower leg, ankle, and foot. For billing, the note should also describe wound depth, bleeding, closure, irrigation, antibiotics, tetanus review, and infection status when relevant.
Right Thigh Dog Bite ICD 10
The ICD-10 code for right thigh dog bite is S71.151A when the dog bite caused an open bite wound of the right thigh during active treatment. ICD-10-CM code references describe S71.151A as open bite, right thigh, initial encounter.
This code should be used only when the bite is on the upper leg/thigh area. If the dog bite is on the shin, calf, or lower leg, the correct code comes from the S81 category instead. Small wording changes matter here. “Right thigh” and “right lower leg” are not the same coding location.
Left Lower Leg Dog Bite ICD 10
The ICD-10 code for left lower leg dog bite is S81.852A for an open bite of the left lower leg, initial encounter. This code applies to dog bite wounds involving the left lower leg area, such as the calf or shin, when documented as an open bite.
For cleaner coding, the provider should avoid writing only “left leg dog bite.” “Left lower leg” gives better support for S81.852A. If the wound is actually on the ankle or foot, the coder should move away from S81 and select the more specific ankle or foot wound category.
Dog Bite Right Leg ICD 10
For a dog bite right leg ICD-10 search, the most common specific code is S81.851A when the wound is an open bite of the right lower leg, initial encounter. ICD-10-CM lists S81.851A for open bite of the right lower leg.
The phrase “right leg” is too broad for strong coding. The provider should document whether the bite is on the right thigh, right lower leg, right ankle, or right foot. For example, S71.151A fits the right thigh, while S81.851A fits the right lower leg. That difference protects the claim from site-specific coding errors.
For most dog bite claims, the clean structure is:
Specific injury code first + W54.0XXA second + infection or complication code when documented.
W54.0XXA: Common Coding Mistakes
One big mistake is using the wrong primary diagnosis, which means that W54 is incorrectly reported as the main diagnosis. Another problem is not having enough information about the external cause code or using the wrong encounter character.
Errors in processing claims are common when the paperwork is not complete or the body part is not clearly chosen. Incorrect sequencing and coding mistakes raise the risk of denial of payment and delay payment. These situations are commonly reviewed underICD-10 related claim denials to correct coding and prevent revenue loss.
CD-10 Codes Related to the W54
The W54 series has a lot of codes that are used at different points in care. W54.0XXD is used when someone is bitten by a dog again. W54.0XXS is for the effects of being bitten by a dog.
W54.1XXA is for the first time someone is hit by a dog, and W54.8XXA is for other times someone comes into contact with a dog. These codes help with classifying animal encounters and coding for follow-up injuries.
Coding Best Practices
Accurate documentation is the foundation of clean claims. Coders must confirm body site identification, injury severity, and encounter type selection for every dog bite case.
External cause reporting must support medical necessity and billing accuracy. Standardized records improve compliance, audit readiness, and healthcare reimbursement optimization.
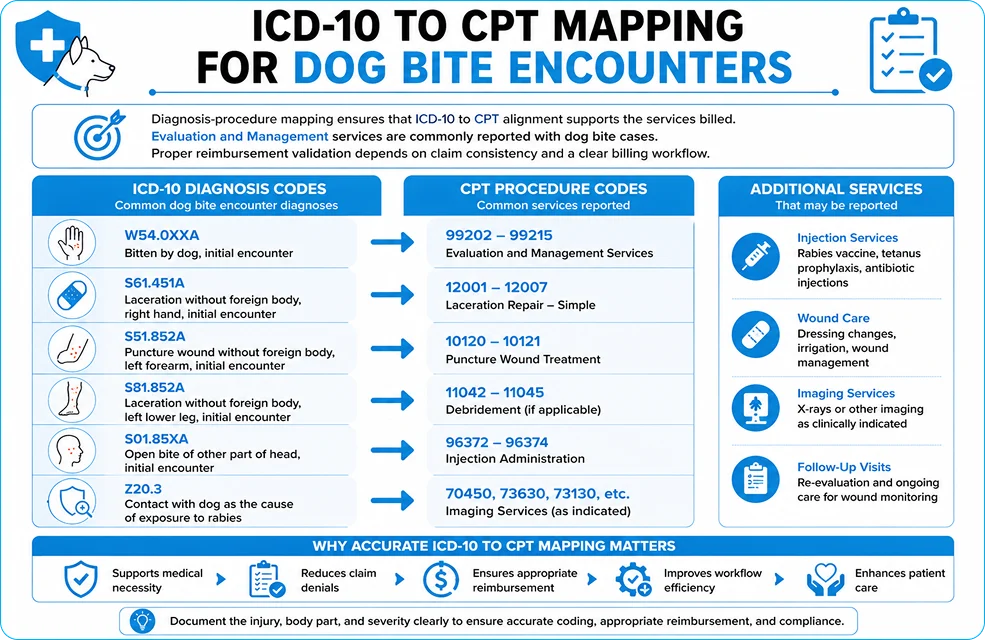
ICD-10 to CPT Mapping for Dog Bite Encounters
Diagnosis-procedure mapping ensures that ICD-10 to CPT alignment supports the services billed. Evaluation and Management services are commonly reported with dog bite cases.
Additional services may include wound repair, laceration treatment, injections, and imaging services. Proper reimbursement validation depends on claim consistency and a clear billing workflow.
Dog Bite ICD-10 Coding Cheat Sheet
W54.0XXA usage depends on the encounter type and body part specificity. Coders must distinguish between the initial encounter, the subsequent encounter, and the sequela encounter.
External cause codes should always support injury documentation. A quick reference guide improves coding accuracy and reduces avoidable errors.
Conclusion
Dog bite ICD-10 codes play a critical role in standardized documentation and accurate injury reporting. Proper use of the W54.0XXA classification supports healthcare coding practices and billing consistency.
Accurate coding improves patient care, reimbursement protection, and statistical injury analysis. By following best practices, healthcare professionals contribute to healthcare research and promote safer patient outcomes.
FAQs:
What is the ICD-10 code for M92.8?
M92.8 is an ICD-10-CM code that stands for “other specified juvenile osteochondrosis.” It is applicable when a particular form of juvenile osteochondrosis is recorded but does not conform to a more specific M92 classification. Accurate clinical documentation is necessary to substantiate its application.
What is the ICD-10 code for M92.8?
ICD-10-CM code M92.8 represents other specified juvenile osteochondrosis conditions. It is used when the disorder is identified but not classified under named osteochondrosis types. Providers should specify the affected site in documentation when possible.
How to code for a dog bite?
Dog bites are coded using the ICD-10-CM code W54.0XXA for an initial encounter. An additional 7th characters are used for subsequent encounters or sequela. An injury code (such as an open wound code) must also be reported to describe the actual injury.What is the ICD-9 code for dog bite, unspecified? The ICD-9-CM code for an unspecified dog bite is E906.0. This code was used to identify dog bite injuries before ICD-10 was implemented. ICD-9 codes are now obsolete for current U.S. medical billing.
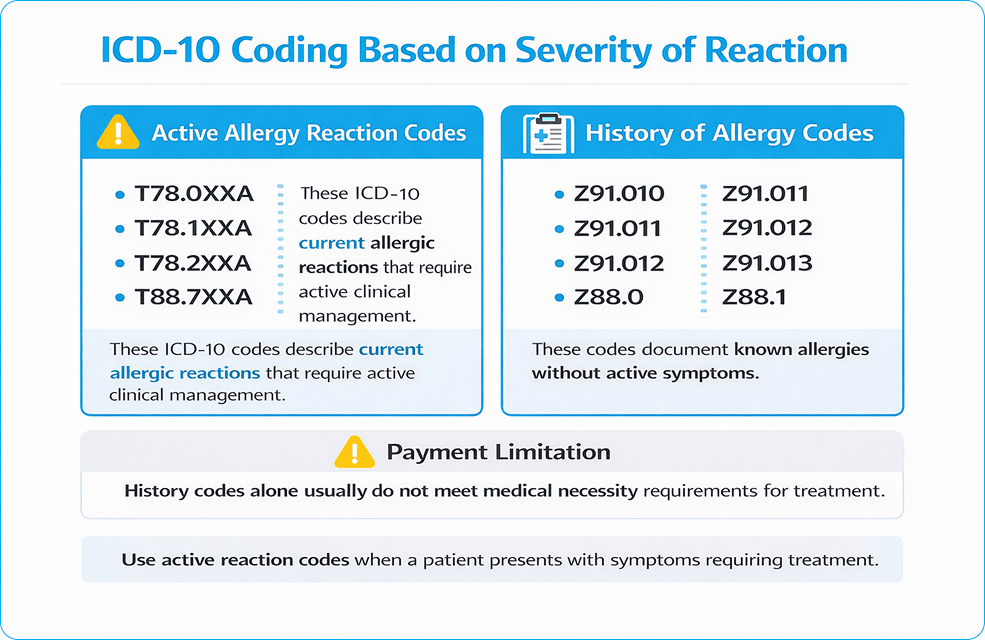
Incorrect ICD-10 coding for allergic reactions triggers denials, delayed payments, and avoidable rework, especially when the trigger is unclear or documentation doesn’t support severity. Errors include using unspecified allergy codes, choosing the wrong T-codes vs. Z-codes, and missing key details like initial vs. subsequent encounter, system involved, and presence of anaphylaxis.
This guide explains how to select the correct ICD-10 code for allergic reactions based on trigger, severity, and encounter type, so claims meet medical necessity and payer editing rules on the first submission.
What is an Allergic Reaction?
Allergic reactions are immune-mediated responses to triggers such as food, medications, insect stings, or environmental exposures. Coding accuracy depends on whether documentation supports a true hypersensitivity/allergic reaction versus a non-immune adverse effect or intolerance.
Clinical notes should clearly document “allergic reaction,” and must document 4 elements:
Trigger (confirmed or suspected)
Severity (mild reaction vs anaphylaxis)
Encounter type (A, D, S when required)
Symptoms and system involvement (skin, airway, GI, cardiovascular)
History of Anaphylaxis vs History of Allergic Reaction ICD-10
Let’s discuss use of the history of codes in allergic reactions.
History of Anaphylaxis ICD-10
Not every patient with a past anaphylactic event is experiencing one today. That’s where history codes come in. A history of anaphylaxis code documents a previous severe allergic reaction that has resolved but remains clinically relevant. Providers often report it when reviewing risk factors, prescribing medications, or assessing future exposure concerns.
History of Allergic Reaction ICD-10
A patient might have a documented allergy history without any current symptoms. History codes help capture those past events in the medical record and alert future providers to potential risks without implying an active allergic condition.
When to Use History Codes vs Active Reaction Codes
The distinction is simple. Historical codes describe something that happened in the past. Active reaction codes describe a condition happening now. A patient with ongoing hives, angioedema, hypersensitivity symptoms, or anaphylaxis requires an active ICD-10 code. A patient whose reaction occurred months or years ago, with no current symptoms or treatment, generally requires a history or allergy status code instead.
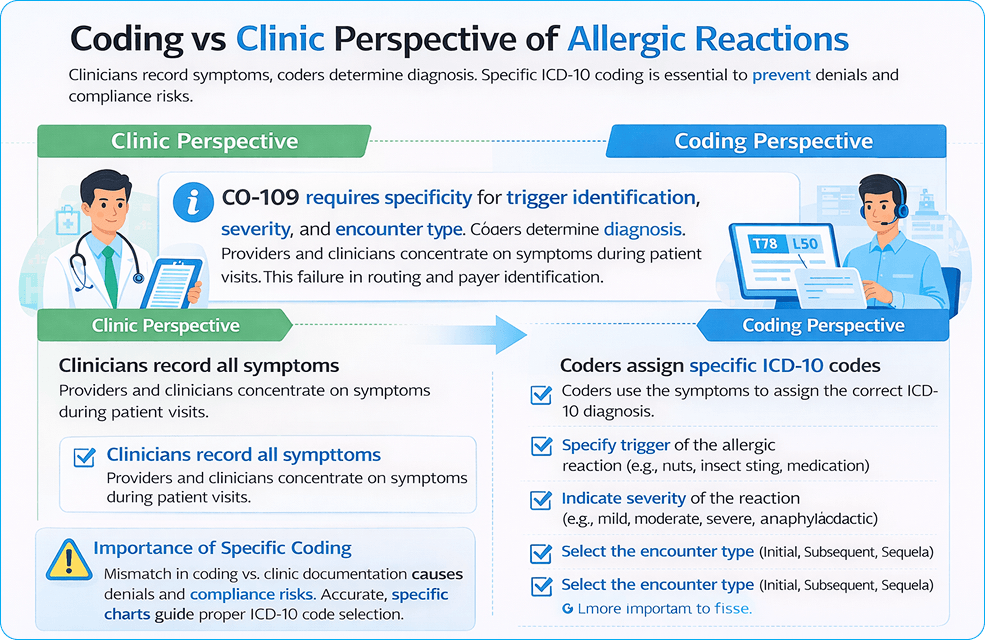
Coding vs Clinic Perspective of Allergic Reactions
Clinicians document symptoms such as urticaria, angioedema, wheezing, throat tightness, and hypotension. Coders convert that documentation into billable diagnosis codes.
Coding accuracy depends on the same 4 data points:
Trigger documented in the assessment
Severity documented in the assessment
7th character present for required codes
Manifestations coded when documented
Coders must identify whether the visit is an initial encounter, a subsequent encounter, or a sequela. Each detail changes code selection and reimbursement impact due to denied claims, payers’ refusal to pay, and compliance risks.
Why is it important to code ICD-10 correctly?
Allergic Reaction ICD-10 coding supports medical necessity and links the diagnosis to the level of service billed. Emergency department and urgent care claims rely on diagnosis specificity for higher-level E/M support. Missing severity and symptom detail weakens the claim when treatment includes epinephrine, IV medications, monitoring, and observation.
Incorrect coding makes payments late, lowers reimbursements, and adds to the workload for administrators. When billing efficiency decreases, healthcare costs increase, and productivity goes down.
ICD-10 Coding Workflow for Allergic Reactions
ICD-10 Coding Workflow for Allergic Reactions
Step 1: Code the Trigger
Identify the allergic reaction trigger (food, drug, insect venom, etc.) to determine the primary code family.
Food: T78.0
Drug: T88.6
Insect: T63.44
Step 2: Code Severity
Determine the severity of the allergic reaction (mild or anaphylaxis).
Minor reaction: T78.4
Anaphylaxis: T78.0, T78.2
Step 3: Add the Encounter Type
Ensure the encounter type is documented (Initial, Subsequent, or Sequela).
Initial encounter: Add code with ‘A’ (e.g., T78.00XA)
Subsequent encounter: Add code with ‘D’ (e.g., T78.00XD)
Sequela: Add code with ‘S’ (e.g., T78.00XS)
Follow these 3 simple steps to ensure accurate coding for allergic reactions, preventing claim denials and reducing delays in reimbursements.
Step 1: Code the trigger category
Trigger selection drives the correct code family. Food, drug, insect venom, contact dermatitis, and unspecified reactions do not share the same primary code logic.
Step 2: Code severity
Anaphylaxis requires separate coding from a mild allergic reaction.
Step 3: Add the encounter type when required
T-codes in injury/poisoning sections require the 7th character for a complete code (A, D, S).
ICD-10 Codes for Specific Allergic Reactions
ICD-10 codes show that a diagnosis is medically necessary and help payers decide if they should pay for it. They tell you why a service was needed and how it relates to the patient’s health.
Allergic Reaction to Hair Dye ICD-10
For allergic reactions to hair dye, the most appropriate ICD-10 code is T78.40XA for an unspecified allergic reaction, initial encounter, unless a specific allergen (e.g., para-phenylenediamine) is identified. If the reaction involves a more specific manifestation, such as contact dermatitis, the code L23.9 (Allergic contact dermatitis, unspecified) may also be relevant.
Allergic Hives ICD-10
Hives, or urticaria, are documented under ICD-10 code L50.9 for unspecified urticaria. If the hives are triggered by a specific allergen, such as a drug or food, more specific codes like L50.0 (Acute urticaria) should be used based on clinical details.
ICD-10 Code for Food Allergy Unspecified
For an unspecified food allergy, the correct ICD-10 code is T78.00XA. This code is used when the food trigger is unknown or not documented, and it represents an allergic reaction to food without specification of the type of food.
Allergy to Sulfa Antibiotics ICD-10
The ICD-10 code for a sulfa drug allergy is Z88.1, which is used to document a history of allergy to sulfonamides. If an acute allergic reaction occurs, it should be coded using T88.6XXA for drug-related anaphylaxis.
ICD-10 Code for Itching Unspecified
For unspecified itching (pruritus), the ICD-10 code L29.9 (Pruritus, unspecified) is used when the cause of the itching is not known or documented. If the itching is due to an allergic reaction or skin condition, additional codes like L50.9 (urticaria) may be used, depending on the presentation.
ICD-10 Environmental Allergies Unspecified
Environmental allergies, if unspecified, would typically fall under T78.40XA, for an unspecified allergic reaction, initial encounter, when there is no known environmental trigger. However, for more specific environmental allergens, codes like Z91.81 (History of hay fever) or Z91.89 (Other specified allergy history) could be used in appropriate contexts.
Hypersensitivity Reaction ICD-10
A hypersensitivity reaction, such as an allergic response to a substance, is often coded under T78.4 (Other adverse effects of drugs, medicaments, and biological substances). If the hypersensitivity reaction involves severe symptoms like anaphylaxis, use T78.0XXA (Anaphylactic reaction due to food) or T78.2XXA (Anaphylactic shock, unspecified trigger) as appropriate.
Strawberry Allergy Status ICD-10
The allergy status for strawberries can be documented under Z91.018 (Other food allergy status). This code is used when a patient has a known history of a strawberry allergy, but the allergy is not currently causing an active reaction. For active allergic reactions, use T78.00XA for unspecified food allergies or a more specific code if known.
Hereditary Angioedema ICD-10
Hereditary angioedema is documented with the ICD-10 code D84.1 (Hereditary angioedema). This condition involves recurring episodes of swelling, often triggered by stress, infections, or trauma. It’s a genetic condition distinct from acute allergic reactions and requires specific coding for diagnosis.
Delayed Hypersensitivity Reaction ICD-10
A delayed hypersensitivity reaction, such as a skin reaction to a drug or toxin, is coded under L23.8 (Allergic contact dermatitis due to other agents). For delayed reactions where the cause is identified, the appropriate allergy-related code should be added based on the clinical presentation.
ICD-10 Code for Allergy to Prednisone
For an allergy to prednisone or a corticosteroid, the ICD-10 code T88.7XXA (Unspecified adverse effect of drug) should be used if the patient experiences an adverse reaction. If there is a confirmed allergy (immune response), Z88.8 (Other drug/biologic allergy status) may be applied to indicate a history of drug allergy.
Proper coding explains ER utilization and urgent care utilization. It also supports resource justification when higher-level services are billed.
Clinical situation
Primary ICD-10-CM code family
Notes
Unspecified allergic reaction treated now
T78.40XA
“Allergy, unspecified, initial encounter.” Use when the trigger lacks documentation.
Anaphylaxis due to food
T78.00XA (unspecified food) / T78.0-series
Food anaphylaxis belongs to the T78.0 category.
Anaphylactic shock, trigger not identified
T78.2XXA
Use when documentation supports anaphylaxis, but the trigger stays undocumented.
Angioedema documented
T78.3XXA
Add when angioedema is documented.
Urticaria documented
L50.9 (or a more specific L50 code)
Add when hives are documented.
Allergic contact dermatitis
L23.9 (or specific L23 code)
Use when contact dermatitis is documented.
Anaphylaxis due to the correct drug properly administered
T88.6XXA
Use for drug-related anaphylaxis due to the adverse effect of the correct drug.
Anaphylaxis due to vaccination
T80.52XA
Use when a vaccination reaction meets anaphylaxis documentation.
Drug Allergy Status ICD-10 Codes (Z88 Series)
Drug allergy status codes identify documented medication allergies when no active allergic reaction is present. These codes communicate important safety information, reduce prescribing risks, and help providers avoid medications that previously caused adverse reactions.
Penicillin Allergy Status (Z88.0)
Z88.0 reports a documented history of penicillin allergy. The patient is not experiencing a current reaction, but the allergy remains clinically relevant when selecting antibiotics. Common examples include prior reactions to penicillin, amoxicillin, or ampicillin.
Sulfonamide Allergy Status (Z88.2)
Z88.2 indicates a history of sulfonamide allergy. This code is frequently associated with sulfa drug allergies, including reactions to sulfamethoxazole-containing medications such as Bactrim. It should not be used to report an active allergic event.
Analgesic Allergy Status (Z88.6)
Z88.6 identifies a documented allergy to analgesic medications. Ibuprofen, ketorolac (Toradol), aspirin, and other pain-relieving drugs may fall into this category when supported by the medical record. The code reflects allergy status rather than a current hypersensitivity reaction.
Other Drug Allergy Status (Z88.8)
Some medication allergies do not fit within a more specific Z88 category. Antihistamines such as diphenhydramine (Benadryl), corticosteroids such as prednisone, or less common medication allergies may be captured using Z88.8 when appropriately documented. Careful provider documentation remains essential to support code selection.
Food Allergy Status ICD-10 Codes (Z91.01 Series)
Food allergy status codes document known food allergies when no active allergic reaction is present. They serve as long-term risk indicators in the medical record. Different purpose. Different coding logic. If a patient arrives with hives, angioedema, or anaphylaxis, an active reaction code is required instead.
Peanut Allergy Status ICD-10 (Z91.010)
Z91.010 identifies a documented peanut allergy. A patient may have experienced a prior allergic reaction, severe sensitivity, or even anaphylaxis related to peanut exposure. The code reflects allergy status only, not a current allergic event.
Milk Allergy Status ICD-10 (Z91.011)
Z91.011 reports a history of milk allergy. This differs from lactose intolerance, which involves digestive symptoms rather than an immune-mediated allergic response. Clinical documentation should clearly establish the allergy diagnosis.
Egg Allergy Status ICD-10 (Z91.012)
Z91.012 is assigned when a patient has a documented allergy to eggs or egg-containing products. The code is commonly reported in preventive care, medication reviews, and immunization-related encounters where allergy history affects clinical decisions.
Seafood Allergy Status ICD-10 (Z91.013)
Z91.013 captures a history of seafood allergy. Fish, shellfish, or multiple seafood-related triggers may be involved. Severity varies widely. Some patients report mild reactions. Others carry a significant risk of anaphylaxis after exposure.
Other Food Allergy Status ICD-10 (Z91.018)
Not every food allergy has its own dedicated ICD-10 code. Z91.018 covers other specified food allergies, including reactions to tree nuts, wheat, soy, sesame, fruits, vegetables, or less common dietary triggers. When searching for an ICD-10 code for allergies, this code frequently appears for food allergies that fall outside the more specific Z91.01 categories.
T-Codes vs Z-Codes in Allergy Claims
T-codes represent an active condition treated now. Z-codes represent allergy status or history.
Z-codes that represent history/status (not acute treatment)
Z-codes document allergy history and status, not an active allergic reaction. In allergy billing, these codes fall into three groups: drug allergy status (Z88), food allergy status (Z91.0), and insect allergy status (Z91.03). Use them to support the record when history is relevant, and pair them with T-codes when the visit involves active treatment.
Allergy history
ICD-10-CM code
Peanut allergy status
Z91.010
Milk allergy status
Z91.011
Egg allergy status
Z91.012
Seafood allergy status
Z91.013
Other food allergy status
Z91.018
Penicillin allergy status
Z88.0
Other Antibiotic allergy status
Z88.1
Sulfonamide allergy status
Z88.2
Other anti-infective allergy status
Z88.3
Analgesic allergy status
Z88.6
Other drug/biologic allergy status
Z88.8
Insect allergy status: BEE
Z91.030
Other insect allergy status
Z91.038
Claim rule: Z-codes do not support medical necessity for an acute allergic reaction visit when used as the only diagnosis.
T-Codes = Active allergic reaction treated during the visit
Active Allergic Reaction – T78 Category
Condition documented
ICD-10-CM code
Anaphylactic reaction due to food
T78.0XXA
Other adverse food reaction (non-anaphylaxis)
T78.1XXA
Anaphylactic shock, unspecified trigger
T78.2XXA
Angioneurotic edema (angioedema)
T78.3XXA
Allergy, unspecified
T78.40XA
Use when: The patient is actively treated for an allergic reaction in ED, urgent care, or office.
Drug-Related Allergic Reactions
Condition documented
ICD-10-CM code
Anaphylaxis due to the correct drug properly administered
T88.6XXA
Unspecified adverse effect of the drug
T88.7XXA
Generalized skin eruption due to a drug
L27.0
Dermatitis due to drug taken internally
L27.1
Use when: Documentation shows immune-mediated drug allergy, rash, or anaphylaxis.
Adverse Drug Reaction vs True Drug Allergy
True drug allergies involve an immune response and hypersensitivity.
Expected side effects and intolerance are not allergies.
Insect Venom Allergic Reactions (Active Sting)
Venom source
ICD-10-CM code family
Bee venom
T63.44–
Wasp venom
T63.46–
Hornet venom
T63.45–
Use when: Patient treated for an active insect sting reaction.
Bee Sting Allergy ICD-10 Codes
Bee sting allergy coding depends on one question: Is the patient having a reaction right now, or is the allergy simply part of their medical history? The answer determines whether an active injury/reaction code or a history code should be reported.
Active Bee Sting Allergic Reaction Coding
An active bee sting allergic reaction requires a code that reflects the current condition being evaluated or treated. Local swelling, urticaria, angioedema, hypersensitivity reactions, and anaphylaxis are coded based on the documented symptoms and severity. The bee sting itself and the resulting allergic response may both affect code selection.
Bee Sting Allergy History Coding (Z91.030)
Z91.030 identifies a personal history of bee sting allergy when no active reaction is present. The patient may have experienced a prior allergic reaction or anaphylactic event after a bee sting, but the condition is not currently being treated. This code serves as a long-term risk indicator and helps alert providers to potential future exposure concerns.
Multiple Drug Allergies ICD-10 Coding
Some patients have a single documented drug allergy. Others have a long list. Penicillin. Sulfonamides. NSAIDs. Contrast agents. The coding challenge is making sure every clinically relevant allergy is captured accurately without overstating the patient’s condition.
Coding Multiple Drug Allergy Status
Multiple drug allergies are typically reported using the appropriate allergy status codes that correspond to each documented medication category. The goal is specificity. A chart that identifies allergies to both penicillin and sulfonamides provides far more clinical value than a vague note stating “multiple drug allergies.”
When Multiple Z88 Codes Can Be Reported
More than one Z88 code may be assigned when a patient has documented allergies involving different drug classes. For example, a patient with a penicillin allergy and a sulfonamide allergy may require both status codes. Each reported code should represent a distinct, documented medication allergy rather than duplicate information.
Documentation Requirements for Multiple Drug Allergies
Details matter. The medical record should identify the specific medication, drug class, or allergy category whenever possible. Providers should clearly distinguish confirmed allergies from side effects, intolerances, or undocumented patient concerns. Strong documentation supports accurate ICD-10 code selection and reduces confusion during future prescribing decisions.
Other ICD-10 codes
Skin/Manifestation Codes (Add when documented)
Manifestation
ICD-10-CM code
Urticaria (hives)
L50.9/L50.8 (or specific L50)
Atopic dermatitis (allergic eczema)
L20.9
Allergic contact dermatitis due to plants
L23.7
Allergic contact dermatitis due to metals
L23.0
Allergic contact dermatitis due to chemicals
L23.5
Allergic contact dermatitis
L23.9/ L23.8 (or specific L23)
Irritant contact dermatitis
L24.9
Generalized skin eruption due to a drug
L27.0
Dermatitis due to a drug taken internally
L27.1
These codes support severity and treatment intensity.
Rule: T-codes explain why treatment was required (E/M, epinephrine, IV meds, monitoring, observation).
Localized Hypersensitivity and Angioedema
Condition documented
ICD-10-CM code
Angioedema (allergic swelling)
T78.3XXA
Lip swelling / localized mucosal swelling
K13.0
Use rule: Add when swelling is documented as part of the allergic reaction.
Vaccine-Related Allergic Reactions
Vaccine reactions belong to the T80–T88 complication category, not T78.
Condition documented
ICD-10-CM code
Infection following immunization
T88.0XXA
Other complications following immunization
T88.1XXA
Complication of immunization, unspecified
T88.9XXA
Anaphylaxis due to vaccine
T80.52XA
Hereditary and Immune-Related Allergic Conditions
These are chronic immune disorders, not acute allergic reactions.
Condition
ICD-10-CM code
Hereditary angioedema
D84.1
Immunodeficiency with antibody defects
D80.0, D80.1
Common variable immunodeficiency
D83.0, D83.1
Immune disorder, unspecified
D84.9, D89.9
Use rule: These codes apply when the visit addresses the immune disorder itself, not an acute allergy event.
Immunization and status support codes
Documentation purpose
ICD-10-CM code
Immunization was not carried out due to an allergy
Z28.82
Immunization was not carried out due to the patient’s refusal
Z28.21
Under-immunization status
Z28.3
Encounter for immunization
Z23
Correct pairing for real claims
Scenario
Correct coding pattern
Patient treated for food-triggered anaphylaxis
T78.0- + (L50.9 if hives documented) + Z91.01x (if known history)
Patient treated for bee sting reaction
T63.44- + manifestation code if documented + Z91.030 (history)
The patient arrives with an unknown allergic reaction
T78.40XA + manifestation codes
Patient follow-up visit with no active reaction
Z91- / Z88- only
7th Character Rules (A, D, S) for Allergy-Related T-Codes
Many allergy-related T-codes require the 7th character for a complete billable code. Missing the 7th character creates an incomplete code and triggers payer rejection.
7th character
Meaning
Typical use
A
Initial encounter (active treatment)
ED evaluation, urgent care evaluation, active workup
D
Subsequent encounter
Follow-up during the recovery phase
S
Sequela
Residual condition linked to a past reaction
Unspecified Allergic Reaction (T78.40XA)
When the allergen is not known at the time of care, an unspecified allergic reaction is reported. Use T78.40XA in 3 situations:
The trigger lacks documentation in the assessment
First-time reaction with no confirmed cause documented
Emergency presentation where the trigger is unknown at the time of service
When to Code Anaphylaxis as a Separate Issue
Anaphylaxis causes reactions that can kill you. It is important to keep track of multi-system involvement, low blood pressure, and airway compromise.
T78.0XXA, T78.2XXA, T78.6XXA, and T80.52XA are ICD-10 codes for anaphylaxis.
Coding based on severity is very important. Documentation must explain how resources are being used.
How to Document Unspecified Codes
Record any symptoms like swelling, wheezing, or a rash.
Please write down any suspected triggers or allergens that you don’t know about.
Record diagnostic tests, labs, and clinical evaluations.
Why Claims are Denied for Allergic Reactions
Allergy claims are denied when the ICD-10 selection does not match what the chart documents. Payers check specificity, severity, and code structure before payment.
8 denial triggers payers flag:
Unspecified code used despite available detail Repeated use of T78.40XA when the trigger, symptoms, or severity are documented.
Wrong primary diagnosis (Z-code misuse) Using Z88 / Z91 as the primary diagnosis instead of an active reaction code (T78 / T88 / T63).
Missing 7th character on T-codes Omitting A / D / S creates an incomplete code and triggers rejection.
Severity not reflected in coding Anaphylaxis, angioedema, urticaria, or respiratory distress documented but not coded.
Manifestations not coded Hives, dermatitis, swelling, or airway symptoms are present in notes but absent in the diagnosis list.
Diagnosis does not match treatment Epinephrine, IV antihistamines, steroids, monitoring, or observation without a severity-supported diagnosis.
Trigger not documented Food, drug, insect sting, or contact exposure not recorded when clinically relevant.
Incomplete clinical notes Missing symptoms, suspected cause, severity, response to treatment, and encounter type.
How to Prevent Allergy Coding Errors Before Claim Submission
Allergy claim accuracy depends on matching the diagnosis to the documented trigger, severity, and treatment. Denial prevention starts during chart review.
Pre-submission prevention steps (8):
Select an active reaction code first Use T78 / T88 / T63 / T80 for visits with active treatment.
Use Z-codes as supporting history only Add Z88 / Z91 when allergy status matters, not as the primary diagnosis.
Capture the trigger in the assessment Document food, drug, insect sting, contact exposure, or unknown trigger.
Capture severity in 1 clear line Document mild reaction, airway symptoms, hypotension, or anaphylaxis.
Add manifestations that appear in the note Code urticaria, angioedema, dermatitis, respiratory symptoms when documented.
Confirm the 7th character on T-codes Use A / D / S where required. Claims reject without it.
Match treatment to diagnosis severity Epinephrine and monitoring require severity documentation.
Avoid repeated unspecified coding patterns Limit T78.40XA when the chart contains trigger or symptom detail.
Emergency Allergic Care Billing
Looking for professional help with billing for emergency allergic reactions? Our experts provide comprehensive services to manage the complexities of emergency medicine billing, including allergenic emergencies.
Accurate ICD-10 allergy coding comes down to matching the diagnosis to what the chart actually proves: trigger, severity, encounter type, and documented manifestations. Start with an active reaction code (T78/T88/T63/T80), add the 7th character when required, and use Z-codes only as supporting history, not as the primary diagnosis for acute treatment. When documentation supports anaphylaxis, code it explicitly and align the diagnosis with interventions like epinephrine, IV meds, monitoring, and observation. Use the workflow and checklist in this guide before submission to reduce denials, shorten A/R time, and keep allergy claims compliant.
FAQs
What is the ICD-10 code for an allergic reaction?
ICD-10 code T78.40XA is used for an unspecified allergic reaction.
What is the ICD-11 code for an allergic reaction?
KA00 is an ICD-11 code for an allergic reaction.
Which ICD-10 codes are required for food allergies related to anaphylaxis?
T78.00XA code is applicable for unspecified food allergy.
Why do allergy-related medical claims get denied by insurance payers?
Allergy-related medical claims are denied because of incomplete diagnosis, incorrect documentation, or wrong code selection.
Incorrect insomnia coding triggers claim edits, medical-necessity requests, denials, and delayed reimbursement. Insomnia coding works best when the diagnosis is clearly supported in the assessment and treatment plan, and the selected ICD-10-CM code matches the documented cause.
This guide explains:
How insomnia is defined clinically
Which ICD-10-CM codes apply to common insomnia scenarios
How to code insomnia with comorbid medical or mental health conditions
What is Insomnia?
Insomnia is a sleep disorder involving difficulty falling asleep, staying asleep, or getting good-quality sleep, even with adequate opportunity and a supportive sleep environment. Daytime impairment appears as fatigue, sleepiness, reduced focus, or functional disruption.
Chronic insomnia is commonly defined as symptoms occurring at least three nights per week for at least three months.
What are the ICD-10 Codes?
ICD-10 codes (International Classification of Diseases, 10th Revision) are standard codes that doctors use to describe diseases, symptoms, and conditions.
In medical billing, these codes are used to show that something is medically necessary to support treatment plans. These codes also help to decide if insurance claims should be paid.
Why Understanding Insomnia ICD-10 Codes Is Important
Different sleep disorders require different ICD-10 codes, so the diagnosis must be specific in the assessment. So, the doctor and medical billers need to be very clear about the patient’s condition when filling out claim submission and reimbursement forms. Correct insomnia coding makes sure you get paid correctly and on time.
In my experience, with the right codes and documentation, not only does the number of claim approvals increase, but it also helps provide better care for patients. Insomnia is a sign of a mental health, neurological, or medical problem, so accurate coding helps payers figure out if insomnia is the main problem or just a sign of another one.
Learning about ICD-10 codes for insomnia and understanding when to use primary vs. comorbid codes makes claims much more accurate and saves both money and time.
Types of Insomnia with respect to Coding
Coding decisions depend on the cause and clinical positioning in the note.
Primary insomnia
Primary insomnia appears as an independent diagnosis with documentation showing insomnia as the primary treatment focus and not attributable to another condition.
Insomnia due to a medical condition
Insomnia links to a documented medical cause (examples: chronic pain disorder, cardiopulmonary disease, endocrine disorder, neurologic disorder). Documentation must state the causal relationship.
Insomnia due to a mental disorder
Insomnia links to a documented mental health cause (examples: major depressive disorder, generalized anxiety disorder, PTSD). Documentation must state the causal relationship and reflect active management.
Comorbid insomnia
Comorbid insomnia exists alongside another condition and requires coding based on what the clinician documents:
Insomnia as a separately treated problem
Insomnia as a symptom or consequence of the primary condition
Insomnia as a factor worsening the primary condition
Primary ICD-10 Codes
These are the most commonly used codes for insomnia:
ICD-10 Code
Description
Use of Code
G47.00
For unspecified insomnia
When the specific cause or type of insomnia is not identified.
G47.09
Other insomnia
Used for specific types of insomnia that are not classified in G47 codes.
G47.01
Insomnia because of any medical condition
When insomnia is linked to a known medical issue.
F51.05
When any mental disorder is a cause of insomnia
Used for known mental health reasons that lead to insomnia
F51.01
Primary insomnia
Insomnia exists independently, but not by any other condition
Comorbid ICD-10 Codes
These are the codes applicable to cases in which insomnia is present along with any other medical condition.
ICD-10 Code
Description
Use of Code
F32.9
Unspecified major depressive disorder, one episode
Depression frequently disrupts sleeping patterns and causes chronic insomnia.
G47.33
Adults with obstructive sleep apnea
Sleep apnea is commonly associated with insomnia, which requires dual coding.
F41.1
Generalized anxiety disorder
Anxiety can result in insomnia by making it difficult to fall or stay asleep.
R53.83
Additional fatigue
Chronic fatigue is a frequent occurrence with sleep disorders, including insomnia.
M79.7
Fibromyalgia
Secondary insomnia is frequently caused by pain-related disorders such as fibromyalgia.
Transition from ICD-9 to ICD-10
Transition from ICD-9 to ICD-10 is required when a case of limited and less diagnosed insomnia shifts to a more detailed and specific diagnosis.
ICD-9 Code
Description
Use of Code
ICD-10 Code for this
307.41
Issues with starting or staying asleep in the short term
A medical condition causing insomnia
G47.01
307.42
A disorder that persists in starting or keeping sleep
Additional sleeplessness
G47.09
327.01
Sleeplessness as a result of a disease
A medical condition causing insomnia
G47.01
780.52
Unspecified sleeplessness
Insomnia, unspecified
G47.00
Coding Guidelines and Exclusion Notes
To code insomnia correctly, you need to read the ICD-10 guidelines very carefully. Coders need to check if insomnia is primary or secondary and make sure that the code matches the clinical assessment of a doctor. A lot of the time, denials happen because the documentation is wrong or exclusion notes are ignored.
Understanding Exclude 2 Notes
Notes that say “Exclude 2” mean that both conditions can be coded together in one documentation. This is the case when insomnia is present with other mental health or medical problems.
Documentation Requirements for Accurate Coding
The following are the major requirements for precise documentation:
A clear diagnosis of insomnia should be documented
What kind of insomnia is it, and why does it happen in detail
If it’s secondary, make sure to connect it clearly to the underlying medical condition.
Describe the period and severity of insomnia
Note symptoms and complications that occur together.
Note the healthcare provider’s clinical assessment that explains why insomnia needs to be treated
Write down the management plan to show that active treatment is required
Ensure that the diagnosis, assessment, and plan are the same on all the documents.
Conclusion
Accurate insomnia coding depends on etiology-based code selection and documentation that supports medical necessity. Specific coding supported by a clear assessment reduces denials compared to vague diagnosis reporting. Correct pairing with comorbid conditions improves claim clarity, supports reimbursement, and strengthens clinical reporting.
FAQs
Which ICD-10-CM code is commonly used for unspecified insomnia?
G47.00 reports insomnia when documentation supports insomnia but does not specify the type or cause.
Can insomnia and a mental health condition be coded together?
Dual coding can be appropriate when documentation supports both diagnoses and active management and excludes notes that do not prohibit pairing.
Is insomnia always a primary diagnosis?
Insomnia may be primary or attributed to a medical or mental health condition based on the clinician’s assessment and documented linkage.
Why do insomnia claims get denied?
Denials follow a diagnosis-to-documentation mismatch, unspecified coding without supporting detail, missing linkage for cause-based codes, or insufficient evidence of medical necessity.
How does ICD-10-CM improve insomnia billing compared to ICD-9?
ICD-10-CM offers more specific insomnia categories and supports clearer cause-based selection, which improves claim clarity when documentation matches the chosen code set.